SOAP vs. DAP Notes: A Side-By-Side Comparison
You’ve got the freedom to choose the note format that fits you — not just the template.
So… what is the difference between SOAP and DAP?
Both are standard progress note formats widely used in healthcare, but SOAP notes sometimes get a bad rap: too slow, too rigid, too old-school.
Meanwhile, DAP notes are seen as the faster, more flexible choice — especially in therapy or high-volume workflows.
But it’s not that simple.
If you’re considering SOAP vs. DAP notes, I’ve broken down the differences in full below. here’s a quick-glance SOAP vs. DAP comparison to ground you.
Why the right note format matters
Clinicians write millions of notes each year. Many outpatient clinicians see roughly
15–25 patients per day and work around 200 clinical days per year, implying 3,000–5,000
encounters annually if each encounter generates at least one progress note.
That’s a lot of paperwork. The right structure can save time, reduce errors, and keep you compliant with legal standards.
SOAP notes overview
The Subjective‑Objective‑Assessment‑Plan (SOAP) note has been the backbone of clinical documentation for decades. It separates what the patient says from what you observe, then moves to your clinical reasoning and the next steps.It’s one of the most widely used note formats in healthcare.
Each section breaks down a different part of the encounter:
- Subjective (S): Why the patient came in — what they report, in their own words.
- Objective (O): What you observe — mood, behavior, vitals, physical findings.
- Assessment (A): Your clinical take — diagnoses, differentials, and context.
- Plan (P): What happens next — follow-ups, referrals, meds, care coordination.
For a deeper dive, see our SOAP notes guide.
SOAP note example
You’ll see these progress notes in nearly every specialty — often with customizations based on setting. Here's an example of a SOAP note in a primary care setting:
Patient Information
Patient Name: Maria Lopez
Date: 05/31/2025
Clinician: Dr. James Patel, MD
Visit Type: Follow-up – hypertension management
1. Subjective
Patient reports feeling “lightheaded in the mornings” over the past week. States she’s been taking her prescribed lisinopril 10mg daily but occasionally forgets to eat breakfast before taking it. Denies chest pain or shortness of breath. Reports good medication adherence otherwise and no recent changes in diet or exercise.
“I feel kind of dizzy when I get up too fast. It’s worse when I haven’t eaten anything.”
2. Objective
BP: 98/64 mmHg
HR: 72 bpm
Temp: 98.4°F
Respirations: 16/min
Weight: 158 lbs (no change)
Cardiovascular: regular rhythm, no murmurs
Neurological: normal gait, no focal deficits
3. Assessment
- Mild hypotension, likely due to lisinopril taken without food
- Hypertension otherwise well-managed
- No signs of acute pathology
- Patient demonstrates good insight into medication timing
4. Plan
- Instructed the patient to consistently eat before taking morning medication
- Continue lisinopril 10mg daily
- Monitor BP at home 3x/week; bring log to next visit
- Follow up in 4 weeks
📌 Read more: How One Rural Clinic Got Back a Full Business Day (10+ hours) Each Week
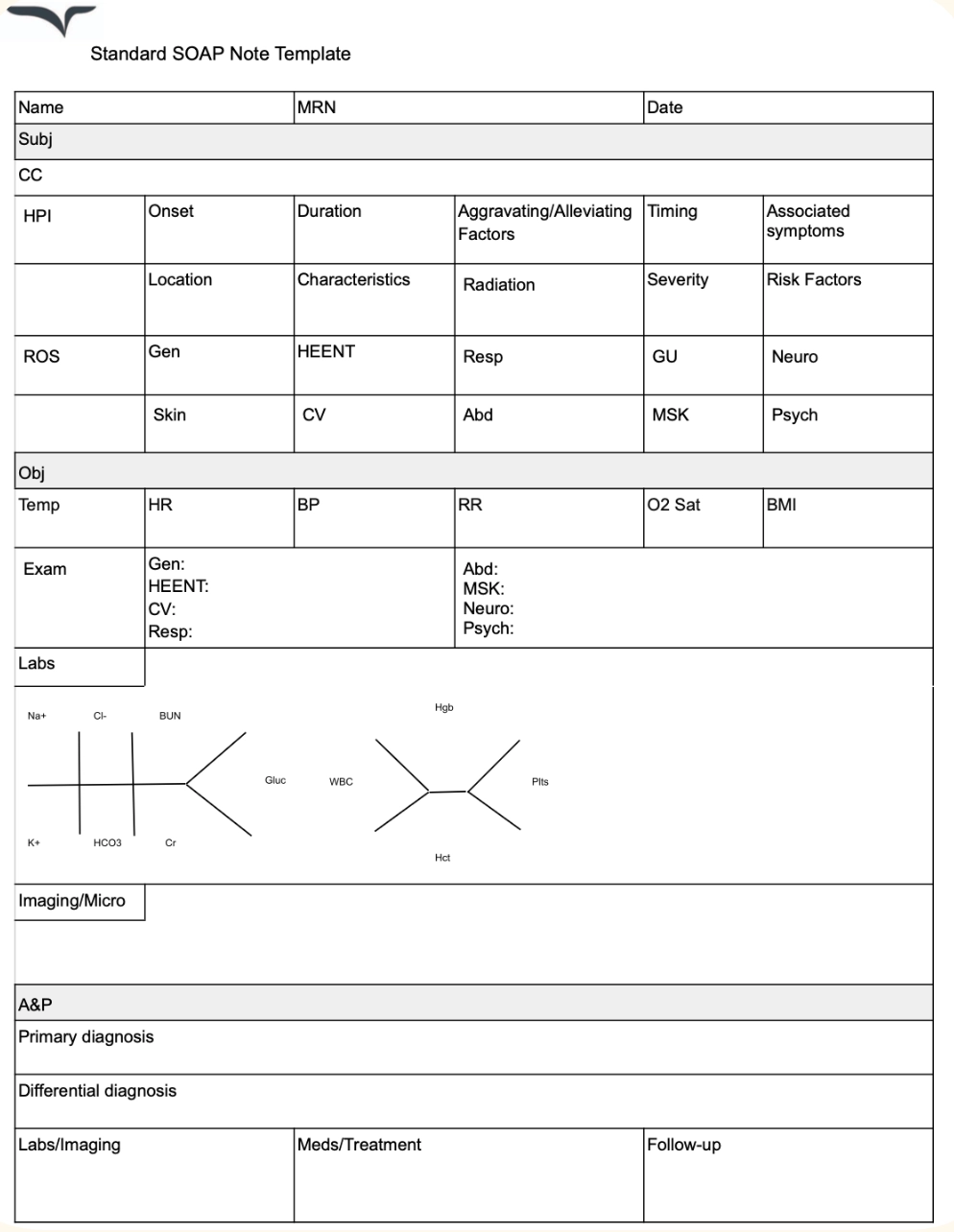
SOAP note template
Here’s a SOAP note template you can adapt to your specialty or workflow.
When to use SOAP notes
These progress notes work best in settings where details matter — like medical decision-making or regulatory documentation.
- Primary care
- Internal medicine
- Any setting where medical decision-making is central
- When required for billing and regulatory documentation (e.g., CMS guidelines)
Do SOAP notes meet regulatory compliance standards?
SOAP and compliance go hand in hand. The structure makes it easier to support audits, billing, and medical necessity documentation. This format must meet HIPAA, state privacy laws, and accreditation standards. Auditors look for clear documentation of what was done, why, and how it will be followed up.
This structure supports audits, insurance claims, and billing documentation, particularly in medical specialties that require detailed justification for procedures or follow-up care.
Why SOAP might be the right fit:
- Built into most EHRs: Most systems already have SOAP templates built in, so they fit right into your usual charting routine.
- Support compliance: The structure checks the right boxes for CMS and insurance purposes — helpful for billing, audits, and staying on the safe side legally.
- Separate what the patient says from what you observe: This is especially useful when your decisions rely on both perspectives.
- Keep care consistent in multi-provider settings: They make it easy for other healthcare professionals to quickly review what’s been done, what was observed, and what the plan is.
- Work across specialties: SOAP can flex to fit different fields, whether you’re in primary care, physical therapy, or mental health.
- Take a little longer to write: Because you’re documenting in four distinct sections, SOAP notes can be more time-consuming.
💡Prefer SOAP but not the time it takes? AI scribes like Freed generate real-time SOAP notes from your visits — customized to your style, ready to upload. Try yourself.
DAP notes overview
DAP stands for Data, Assessment, and Plan. It’s a simplified clinical note format commonly used in behavioral health, counseling, and community-based care.
DAP notes are simpler by design — great for fast-paced, relationship-centered care.
DAP notes break into three sections:
- Data (D): A blend of what the client shares and what you observe.
- Assessment (A): Your clinical impression or interpretation of how the session went. This might include client progress toward goals, shifts in mental status, or how the client responded to interventions.
- Plan (P): Next steps — any follow-up, referrals, homework, safety planning, or goals for the next session.
Learn more about DAP notes in our dedicated article: DAP notes overview.
DAP note example
Here’s how this progress note might look in a therapy session:
Patient Information
Client Name: Jordan Rivers
Date: 05/31/2025
Clinician: Taylor Nguyen, LCSW
Session Type: Individual therapy – 8th session
Focus: Coping strategies for anxiety
1. Data
Client discussed recent work stress related to an upcoming deadline and reported increased anxiety symptoms (e.g., restlessness, trouble sleeping, and difficulty focusing). Noted that they attempted breathing exercises once but felt “too busy” to do them consistently. Client became tearful when discussing feeling “not good enough” at work and expressed fear of failure.
“It’s like my brain won’t shut off. Even when I’m tired, I can’t relax.”
2. Assessment
Client continues to experience moderate anxiety symptoms, particularly around performance at work. Some progress in identifying emotional triggers, but limited follow-through with coping techniques. Client appeared emotionally open and engaged throughout the session, with growing insight into self-critical thought patterns.
3. Plan
- Revisit and simplify coping strategies to better fit client's current routine
- Assign short journaling prompt to explore negative self-talk
- Practice 2-minute grounding technique during next session
- Plan to assess sleep and energy levels more closely in future sessions
When to use DAP notes
DAP notes are great for settings where sessions are frequent, progress is tracked over time, and clinical decision-making doesn’t hinge on separating subjective from objective input.
They’re commonly used in:
- Behavioral health and therapy sessions
- Social work and case management
- Substance use treatment
- School counseling
- Community outreach programs
Do DAP notes meet regulatory compliance standards?
These progress notes can still meet compliance standards for medical documentation in many behavioral health orgs — just make sure your structure is consistent.
Just note: DAP may not be accepted in settings that require highly detailed or medically coded documentation.
Why DAP notes might be a better fit:
- Quicker to write: With only three sections, DAP notes are faster to complete — helpful in high-volume practices or back-to-back sessions.
- Reduce over-documentation: DAP notes cut down on unnecessary detail.
- Great for behavioral health: DAP is especially suited for therapy, counseling, and case management, where sessions focus on patterns, goals, and emotional progress over time.
- Flexible structure: The format is less rigid than SOAP and allows you to adapt the depth and style of your notes depending on the session.
- Still support compliance: When used consistently and in alignment with treatment planning, DAP notes can meet documentation requirements for many behavioral health orgs and payers.
- May not work for all settings
If you’re in a medical field or need to justify clinical decisions with detailed objective data, SOAP might be a better fit.
Other popular note types
- BIRP notes: BIRP stands for Behavior, Intervention, Response, and Plan. These are frequently used in behavioral health to document how a client responds to interventions during a session.
- PAIP notes: Short for Problem, Assessment, Intervention, and Plan, PAIP notes are often used in behavioral health, substance use treatment, and case management. They follow a logical flow similar to SOAP but with a bit more flexibility and less emphasis on separating subjective sections and objective data.
- PIE notes: This format — Presentation, Intervention, Evaluation — is popular in acute care settings. It’s a streamlined, action-oriented note style that supports quick, evidence-based documentation, often used by clinicians managing high patient volumes.
- GIRP notes: Standing for Goal, Intervention, Response, Plan, GIRP notes are commonly used in social work and case management. The emphasis here is on tracking progress toward specific treatment goals rather than just behavioral responses.
SOAP or DAP? Which progress note is for you?
Not sure which to choose? Start with your workflow:
When to use SOAP notes
Best for medical providers, psychiatrists, or anyone working in a multi-provider team. They’re especially useful when detailed, structured documentation is important, like when a nurse is tracking vital signs and medication effects after surgery.
When to use DAP notes
Great for behavioral health settings. They’re a good fit when you need a faster, more flexible format, like when a therapist is jotting down key takeaways and next steps after a counseling session.
Best‑practice tips for any note
- Start with a template – saves time and ensures consistency.
- Use bullet points for lists (medications, labs).
- Focus on relevance – include only data that influences assessment or plan.
- Proofread for clarity – a single ambiguous phrase can cause a chart audit flag.
- Leverage technology – AI scribes can auto‑populate sections, leaving you to verify.
Legal compliance and regulations for SOAP and DAP Notes
Clinical documentation must meet specific legal and regulatory standards to support billing, audits, and quality care reviews. The Centers for Medicare & Medicaid Services (CMS) require that documentation clearly justifies the medical necessity of services, is completed promptly (typically within 48 to 72 hours), and includes sufficient detail to support the level of care billed.
Both SOAP and DAP note formats can satisfy these standards when executed thoroughly and consistently. While SOAP’s four-part structure—separating subjective patient input from objective findings—often aligns closely with CMS documentation and billing guidelines, DAP notes may be acceptable in behavioral health or other specialized settings where streamlined notes remain detailed enough to demonstrate clinical decision-making and support claims.
Similarly, accreditation bodies like The Joint Commission emphasize accuracy, completeness, legibility, and authentication of clinical records as core requirements. SOAP notes’ structured approach supports multi-provider communication, facilitating continuity of care and legal defensibility in audits or legal reviews. DAP notes can also fulfill these criteria, provided that the "Data" section combines objective and subjective information clearly and the note’s overall content documents the rationale for treatment and next steps. Importantly, both formats must uphold HIPAA privacy and security regulations, safeguarding patient information throughout documentation and storage.
Technological tools such as electronic health records with templated notes and AI-enabled scribes can support compliance by standardizing documentation quality, minimizing errors, and ensuring timely completion. Ultimately, the choice between SOAP and DAP should consider regulatory requirements, payer expectations, clinical complexity, and workflow efficiency, with consistent application being key to maintaining legal and compliance standards
How Freed can help you master both formats
At the end of the day, progress notes aren’t just a requirement — they’re a reflection of how you think, how you care, and how you communicate across a team.
Whether you choose SOAP, DAP, or something in between, the best format is the one that helps you document clearly, stay grounded in the visit, and still get out the door on time.
That’s the goal. Not more documentation — just better, lighter, smarter documentation that works for you.
And if your notes still feel like the heaviest part of your day? There are tools for that.
Freed’s ambient AI scribe helps clinicians capture the full picture — with structure, nuance, and zero copy-pasting — so you can chart less, and care more.
Ready to see how effortless note‑taking can be? Learn more about Freed’s AI scribe and start a free trial today.
Table of Contents
You’ve got the freedom to choose the note format that fits you — not just the template.
So… what is the difference between SOAP and DAP?
Both are standard progress note formats widely used in healthcare, but SOAP notes sometimes get a bad rap: too slow, too rigid, too old-school.
Meanwhile, DAP notes are seen as the faster, more flexible choice — especially in therapy or high-volume workflows.
But it’s not that simple.
If you’re considering SOAP vs. DAP notes, I’ve broken down the differences in full below. here’s a quick-glance SOAP vs. DAP comparison to ground you.
Why the right note format matters
Clinicians write millions of notes each year. Many outpatient clinicians see roughly
15–25 patients per day and work around 200 clinical days per year, implying 3,000–5,000
encounters annually if each encounter generates at least one progress note.
That’s a lot of paperwork. The right structure can save time, reduce errors, and keep you compliant with legal standards.
SOAP notes overview
The Subjective‑Objective‑Assessment‑Plan (SOAP) note has been the backbone of clinical documentation for decades. It separates what the patient says from what you observe, then moves to your clinical reasoning and the next steps.It’s one of the most widely used note formats in healthcare.
Each section breaks down a different part of the encounter:
- Subjective (S): Why the patient came in — what they report, in their own words.
- Objective (O): What you observe — mood, behavior, vitals, physical findings.
- Assessment (A): Your clinical take — diagnoses, differentials, and context.
- Plan (P): What happens next — follow-ups, referrals, meds, care coordination.
For a deeper dive, see our SOAP notes guide.
SOAP note example
You’ll see these progress notes in nearly every specialty — often with customizations based on setting. Here's an example of a SOAP note in a primary care setting:
Patient Information
Patient Name: Maria Lopez
Date: 05/31/2025
Clinician: Dr. James Patel, MD
Visit Type: Follow-up – hypertension management
1. Subjective
Patient reports feeling “lightheaded in the mornings” over the past week. States she’s been taking her prescribed lisinopril 10mg daily but occasionally forgets to eat breakfast before taking it. Denies chest pain or shortness of breath. Reports good medication adherence otherwise and no recent changes in diet or exercise.
“I feel kind of dizzy when I get up too fast. It’s worse when I haven’t eaten anything.”
2. Objective
BP: 98/64 mmHg
HR: 72 bpm
Temp: 98.4°F
Respirations: 16/min
Weight: 158 lbs (no change)
Cardiovascular: regular rhythm, no murmurs
Neurological: normal gait, no focal deficits
3. Assessment
- Mild hypotension, likely due to lisinopril taken without food
- Hypertension otherwise well-managed
- No signs of acute pathology
- Patient demonstrates good insight into medication timing
4. Plan
- Instructed the patient to consistently eat before taking morning medication
- Continue lisinopril 10mg daily
- Monitor BP at home 3x/week; bring log to next visit
- Follow up in 4 weeks
📌 Read more: How One Rural Clinic Got Back a Full Business Day (10+ hours) Each Week
SOAP note template
Here’s a SOAP note template you can adapt to your specialty or workflow.
When to use SOAP notes
These progress notes work best in settings where details matter — like medical decision-making or regulatory documentation.
- Primary care
- Internal medicine
- Any setting where medical decision-making is central
- When required for billing and regulatory documentation (e.g., CMS guidelines)
Do SOAP notes meet regulatory compliance standards?
SOAP and compliance go hand in hand. The structure makes it easier to support audits, billing, and medical necessity documentation. This format must meet HIPAA, state privacy laws, and accreditation standards. Auditors look for clear documentation of what was done, why, and how it will be followed up.
This structure supports audits, insurance claims, and billing documentation, particularly in medical specialties that require detailed justification for procedures or follow-up care.
Why SOAP might be the right fit:
- Built into most EHRs: Most systems already have SOAP templates built in, so they fit right into your usual charting routine.
- Support compliance: The structure checks the right boxes for CMS and insurance purposes — helpful for billing, audits, and staying on the safe side legally.
- Separate what the patient says from what you observe: This is especially useful when your decisions rely on both perspectives.
- Keep care consistent in multi-provider settings: They make it easy for other healthcare professionals to quickly review what’s been done, what was observed, and what the plan is.
- Work across specialties: SOAP can flex to fit different fields, whether you’re in primary care, physical therapy, or mental health.
- Take a little longer to write: Because you’re documenting in four distinct sections, SOAP notes can be more time-consuming.
💡Prefer SOAP but not the time it takes? AI scribes like Freed generate real-time SOAP notes from your visits — customized to your style, ready to upload. Try yourself.
DAP notes overview
DAP stands for Data, Assessment, and Plan. It’s a simplified clinical note format commonly used in behavioral health, counseling, and community-based care.
DAP notes are simpler by design — great for fast-paced, relationship-centered care.
DAP notes break into three sections:
- Data (D): A blend of what the client shares and what you observe.
- Assessment (A): Your clinical impression or interpretation of how the session went. This might include client progress toward goals, shifts in mental status, or how the client responded to interventions.
- Plan (P): Next steps — any follow-up, referrals, homework, safety planning, or goals for the next session.
Learn more about DAP notes in our dedicated article: DAP notes overview.
DAP note example
Here’s how this progress note might look in a therapy session:
Patient Information
Client Name: Jordan Rivers
Date: 05/31/2025
Clinician: Taylor Nguyen, LCSW
Session Type: Individual therapy – 8th session
Focus: Coping strategies for anxiety
1. Data
Client discussed recent work stress related to an upcoming deadline and reported increased anxiety symptoms (e.g., restlessness, trouble sleeping, and difficulty focusing). Noted that they attempted breathing exercises once but felt “too busy” to do them consistently. Client became tearful when discussing feeling “not good enough” at work and expressed fear of failure.
“It’s like my brain won’t shut off. Even when I’m tired, I can’t relax.”
2. Assessment
Client continues to experience moderate anxiety symptoms, particularly around performance at work. Some progress in identifying emotional triggers, but limited follow-through with coping techniques. Client appeared emotionally open and engaged throughout the session, with growing insight into self-critical thought patterns.
3. Plan
- Revisit and simplify coping strategies to better fit client's current routine
- Assign short journaling prompt to explore negative self-talk
- Practice 2-minute grounding technique during next session
- Plan to assess sleep and energy levels more closely in future sessions
When to use DAP notes
DAP notes are great for settings where sessions are frequent, progress is tracked over time, and clinical decision-making doesn’t hinge on separating subjective from objective input.
They’re commonly used in:
- Behavioral health and therapy sessions
- Social work and case management
- Substance use treatment
- School counseling
- Community outreach programs
Do DAP notes meet regulatory compliance standards?
These progress notes can still meet compliance standards for medical documentation in many behavioral health orgs — just make sure your structure is consistent.
Just note: DAP may not be accepted in settings that require highly detailed or medically coded documentation.
Why DAP notes might be a better fit:
- Quicker to write: With only three sections, DAP notes are faster to complete — helpful in high-volume practices or back-to-back sessions.
- Reduce over-documentation: DAP notes cut down on unnecessary detail.
- Great for behavioral health: DAP is especially suited for therapy, counseling, and case management, where sessions focus on patterns, goals, and emotional progress over time.
- Flexible structure: The format is less rigid than SOAP and allows you to adapt the depth and style of your notes depending on the session.
- Still support compliance: When used consistently and in alignment with treatment planning, DAP notes can meet documentation requirements for many behavioral health orgs and payers.
- May not work for all settings
If you’re in a medical field or need to justify clinical decisions with detailed objective data, SOAP might be a better fit.
Other popular note types
- BIRP notes: BIRP stands for Behavior, Intervention, Response, and Plan. These are frequently used in behavioral health to document how a client responds to interventions during a session.
- PAIP notes: Short for Problem, Assessment, Intervention, and Plan, PAIP notes are often used in behavioral health, substance use treatment, and case management. They follow a logical flow similar to SOAP but with a bit more flexibility and less emphasis on separating subjective sections and objective data.
- PIE notes: This format — Presentation, Intervention, Evaluation — is popular in acute care settings. It’s a streamlined, action-oriented note style that supports quick, evidence-based documentation, often used by clinicians managing high patient volumes.
- GIRP notes: Standing for Goal, Intervention, Response, Plan, GIRP notes are commonly used in social work and case management. The emphasis here is on tracking progress toward specific treatment goals rather than just behavioral responses.
SOAP or DAP? Which progress note is for you?
Not sure which to choose? Start with your workflow:
When to use SOAP notes
Best for medical providers, psychiatrists, or anyone working in a multi-provider team. They’re especially useful when detailed, structured documentation is important, like when a nurse is tracking vital signs and medication effects after surgery.
When to use DAP notes
Great for behavioral health settings. They’re a good fit when you need a faster, more flexible format, like when a therapist is jotting down key takeaways and next steps after a counseling session.
Best‑practice tips for any note
- Start with a template – saves time and ensures consistency.
- Use bullet points for lists (medications, labs).
- Focus on relevance – include only data that influences assessment or plan.
- Proofread for clarity – a single ambiguous phrase can cause a chart audit flag.
- Leverage technology – AI scribes can auto‑populate sections, leaving you to verify.
Legal compliance and regulations for SOAP and DAP Notes
Clinical documentation must meet specific legal and regulatory standards to support billing, audits, and quality care reviews. The Centers for Medicare & Medicaid Services (CMS) require that documentation clearly justifies the medical necessity of services, is completed promptly (typically within 48 to 72 hours), and includes sufficient detail to support the level of care billed.
Both SOAP and DAP note formats can satisfy these standards when executed thoroughly and consistently. While SOAP’s four-part structure—separating subjective patient input from objective findings—often aligns closely with CMS documentation and billing guidelines, DAP notes may be acceptable in behavioral health or other specialized settings where streamlined notes remain detailed enough to demonstrate clinical decision-making and support claims.
Similarly, accreditation bodies like The Joint Commission emphasize accuracy, completeness, legibility, and authentication of clinical records as core requirements. SOAP notes’ structured approach supports multi-provider communication, facilitating continuity of care and legal defensibility in audits or legal reviews. DAP notes can also fulfill these criteria, provided that the "Data" section combines objective and subjective information clearly and the note’s overall content documents the rationale for treatment and next steps. Importantly, both formats must uphold HIPAA privacy and security regulations, safeguarding patient information throughout documentation and storage.
Technological tools such as electronic health records with templated notes and AI-enabled scribes can support compliance by standardizing documentation quality, minimizing errors, and ensuring timely completion. Ultimately, the choice between SOAP and DAP should consider regulatory requirements, payer expectations, clinical complexity, and workflow efficiency, with consistent application being key to maintaining legal and compliance standards
How Freed can help you master both formats
At the end of the day, progress notes aren’t just a requirement — they’re a reflection of how you think, how you care, and how you communicate across a team.
Whether you choose SOAP, DAP, or something in between, the best format is the one that helps you document clearly, stay grounded in the visit, and still get out the door on time.
That’s the goal. Not more documentation — just better, lighter, smarter documentation that works for you.
And if your notes still feel like the heaviest part of your day? There are tools for that.
Freed’s ambient AI scribe helps clinicians capture the full picture — with structure, nuance, and zero copy-pasting — so you can chart less, and care more.
Ready to see how effortless note‑taking can be? Learn more about Freed’s AI scribe and start a free trial today.
FAQs
Frequently asked questions from clinicians and medical practitioners.
What is the difference between DAP and SOAP notes?
Do doctors still use SOAP notes?
What is a DAP note?
What is the difference between a SOAP note and a progress note?
What is the main difference between SOAP and DAP notes?
Is SOAP or DAP better for insurance and billing?
Can I switch between SOAP and DAP depending on the visit?

Related content
Free yourself for better things
548 Market Street, PMB 95301
San Francisco, CA 94104
Specialties
Compliance & Security
Our technology is HIPAA-compliant, uses industry best practices, and doesn’t store patient recordings.