How to Write SOAP Notes: Real Examples + Free Template (2026)
You can defuse a crisis at 10 am, soothe a patient's meltdown at 10:30, and maybe even perform a minor miracle before noon.
But having to catch up on SOAP notes after all that? Sometimes, that's the loose thread that can unravel anyone's sanity.
The SOAP format has been a staple of clinical documentation for over 50 years — but let's face it, it isn't always smooth sailing. Time crunches, juggling consistency, and figuring out what details matter most can leave even seasoned clinicians at a loss.
In this guide, you'll find real SOAP note examples across specialties, a free copy-paste template, and tips from clinicians who've cracked the code on writing notes without sacrificing their evenings.
Want the note written for you? Freed's AI scribe listens to your visit and generates a complete SOAP note in about 60 seconds. Try it free →
What are SOAP notes?
SOAP notes are the tried-and-true format most clinicians use to document patient encounters. SOAP stands for Subjective, Objective, Assessment, and Plan — four sections that organize your findings, clinical reasoning, and next steps into a format any provider can follow.
Here's why the structure matters:
- Improves efficiency: Clinicians can quickly locate key information — reported symptoms, diagnostic findings, care plan — without searching through paragraph-heavy notes. A clear structure also supports legal, billing, and audit requirements.
- Supports clinical decision-making: Separating notes into defined sections helps you present assessments and rationale logically. SOAP notes empower providers to act on clearly documented evidence.
- Enhances patient outcomes: A well-documented SOAP note creates accountability for thorough, actionable care plans. Comprehensiveness with purpose — not aimless length.
- Simplifies standardization: SOAP's consistency sets it apart from other frameworks like DAP (Data, Assessment, Plan). SOAP is precise and evidence-based; DAP is more flexible. For multidisciplinary or evidence-heavy documentation, SOAP wins.
A brief history: Why SOAP notes exist
SOAP wasn't invented by a committee. It came from one clinician who was frustrated enough to build something better.
Larry Weed was both a practicing physician and a research scientist. Standing in both worlds, he saw what medicine lacked: a systematic way to organize clinical thinking.
In his words:
"A physician works in a chaotic system of keeping and organizing data and has no systematic review and correction of his daily work."
So he built one. Weed's problem-oriented medical record, developed in the 1960s, introduced the idea that a clinical note should start with the problem in front of you — not the clinician's impression of it. He wanted data, not bias.
The result was the problem list — and eventually, the SOAP format. It took four years to rearrange how medicine documented patient care, but the framework Weed built became the backbone of modern clinical documentation.
His standard for a good note: thorough, reliable, analytically sound, and efficient. Not longer. Just better.
SOAP note format: what goes in each section
Each section of this type of progress note has a specific purpose in helping clinicians sort their findings, data, and care recommendations.
Here's a quick reference:
Let's break down each section with examples:
Subjective
The subjective section captures a patient’s subjective perspective about their concerns and experiences.
You’ll document the:
- Primary problem (chief complaint) presented in the patient encounter,
- The review of systems (ROS) to see how and if symptoms present
- Other relevant information like medical history or lifestyle habits that could be related to their complaint.
Examples of a Subjective
- Mr. Jones' chief complaint is a back pain. He also exercises 5x a week with heavy weights.
- Angie complained of abdominal pain that has persisted for the past two days.
Helpful tip
If you can't measure or verify it directly, it belongs in Subjective.
Objective
The objective section records of measurable data collected during a patient’s visit, such as physical exam results and laboratory results completed during that time. Physicians will also add their observations or direct patient quotes to this section.
Examples of an Objective
- Mr. Jones' vital signs are normal. His lower back has tenderness to palpation.
- Angie’s abdomen has no rebound tenderness in the lower right quadrant. No visible swelling or bruising.
Helpful tip
Use shorthand where appropriate, but spell out anything a provider outside your specialty might not recognize.
Assessment
This assessment section summarizes the patient’s perspectives and physician observations into a clinical diagnosis.
This section holds the most weight in your SOAP note as it describes a thorough analysis of the patient’s problems, all possible diagnoses, and the reasoning behind that diagnosis.
Examples of an Assessment
- Lower back pain is a lumbar muscle strain from overexertion during heavy weightlifting. A different diagnosis could be a Vitamin D deficiency.
- Abdominal pain without signs of acute abdomen or significant palpation. Likely gastrointestinal discomfort or mild inflammation.
Helpful tip
Don't just name the diagnosis — show the thread.
Plan
The plan section (usually combined with assessment) outlines the next steps in your recommended treatment plan. You’ll use this section to detail information such as action items for future examinations, required medication, or referrals for more testing or consultations with specialists.
Examples of a Plan
- Recommend avoidance of heavy lifting for one to two weeks. Prescribe a mild analgesic for pain and a diagnostic test for D3 deficiency. Schedule a follow-up appointment next week.
- Prescribe over-the-counter antacids for relief when needed. Monitor for symptoms like fever, severe pain, nausea, or vomiting.
Helpful tip:
In many specialties, Assessment and Plan are combined into a single A&P section for efficiency. This is accepted practice.
SOAP note examples (and what you can learn from them)
The examples below will help you better visualize how healthcare providers use the SOAP template to structure and guide their clinical documentation.
We've included both illustrated examples and fully written text examples you can learn from directly.
Example 1: SOAP note for abdominal pain (primary care)
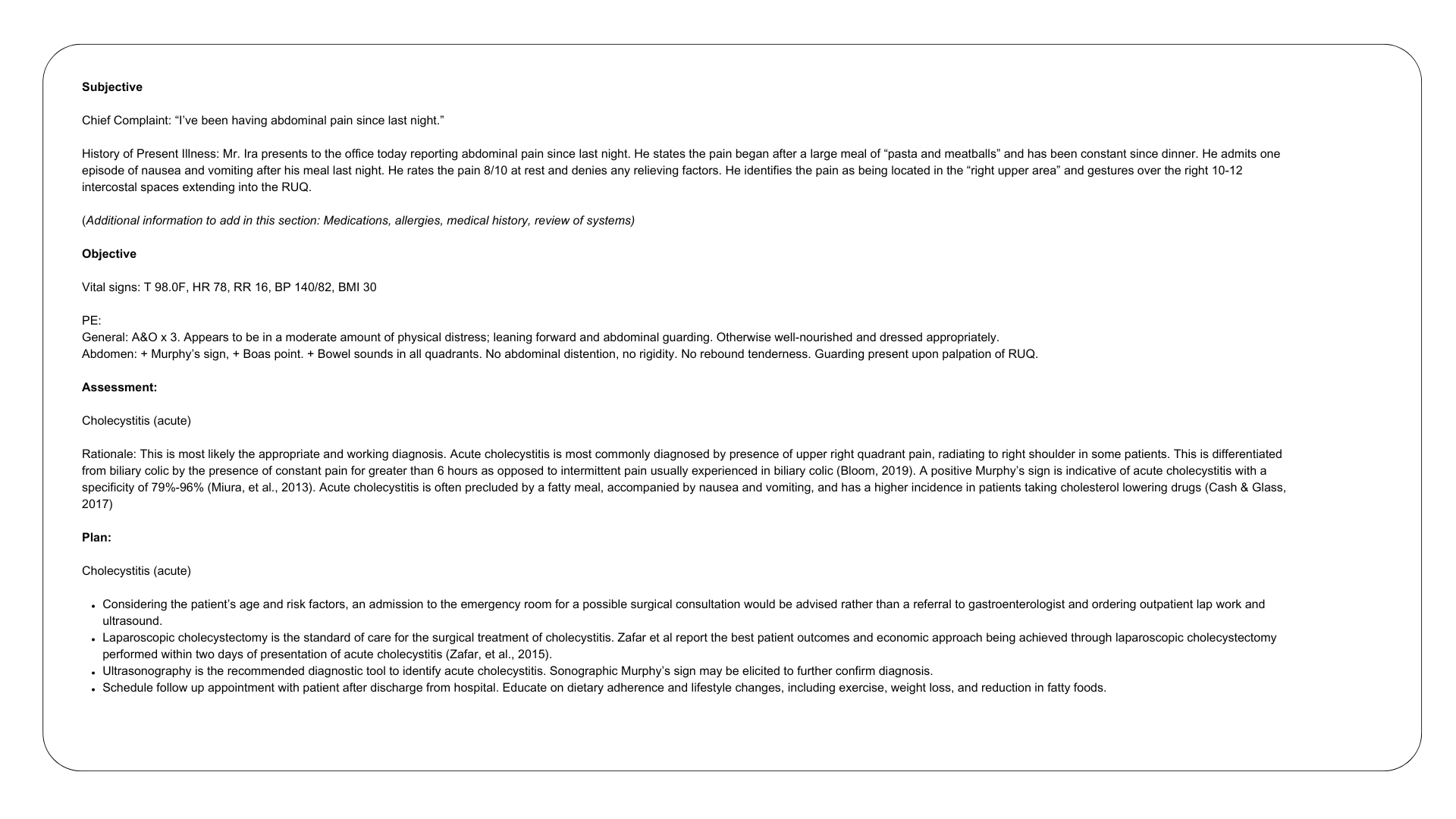
What can we learn from this example?
- It provides a clear timeline with descriptions of symptoms, including patient quotes and relevant anecdotes for clarity.
- It includes vital signs and specific diagnostic indicators for a more precise diagnosis.
- The assessment is supported by clinical findings that differentiate possible conditions and reference relevant literature.
- The document includes clear next steps and provides actionable patient instructions.
Example 2: SOAP note chronic disease follow-up (diabetes management)
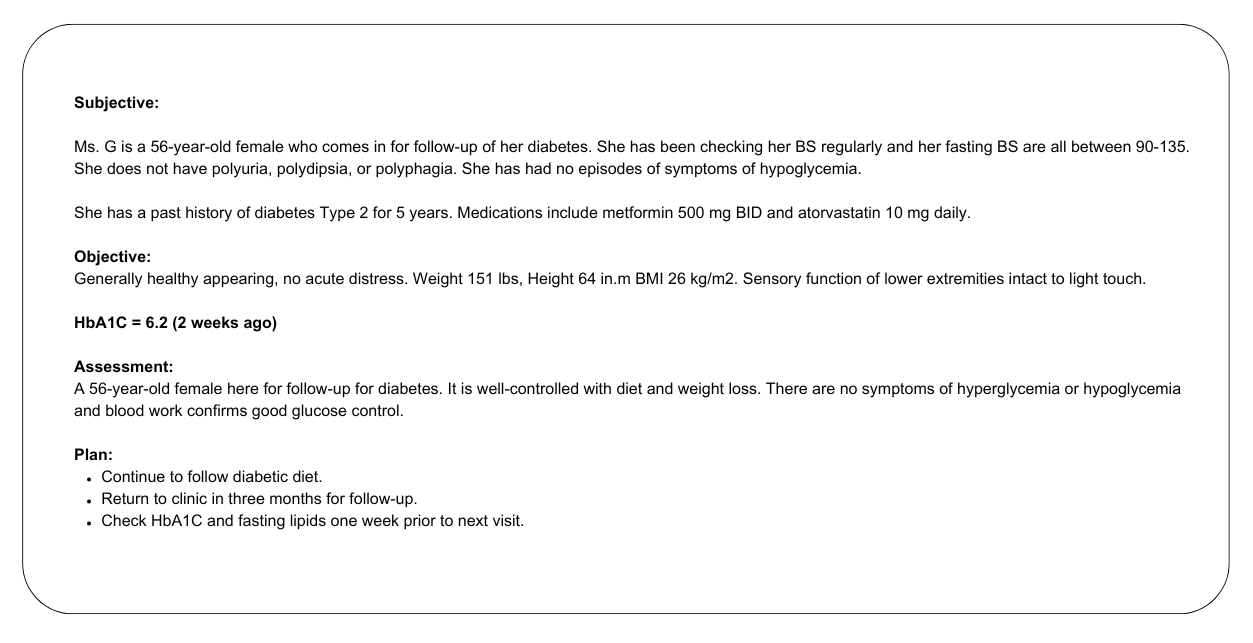
What can we learn from this example?
- The note is concise and avoids unnecessary details, making it easier for healthcare providers to understand the patient’s condition and care plan.
- The patient’s history, symptoms, and self-reported readings are documented because they are relevant to her diabetes management.
- The plan clearly describes ongoing management strategies and outlines appropriate follow-ups, and includes specific instructions for pre-visit tests, laboratory results, and diagnostic results
Get a free, downloadable SOAP note template
6 tips for writing powerful SOAP notes
Beyond understanding the purpose of each SOAP section, clinicians have to approach the note-taking process with a clear understanding of how to optimize their language choices and writing styles specifically for documentation.
Now that you've seen what strong clinical notes look like in action, let's review a few important reminders that reinforce the clarity, effectiveness, and overall efficiency of your medical notes.
Avoid jargon and abbreviations
Remember that SOAP notes aim to help your entire healthcare team ensure accuracy, drive patient care forward, and avoid miscommunication.
Using universal language that multidisciplinary healthcare providers can understand is important in making your documentation readable and easy to act on.
The next provider meeting your patient may be someone outside your specialty. If that’s the case, you’ll want to:
- Do: Explain acronyms the first time you use them if you need to bring that acronym up.
- Don’t: Use shorthand commonly used in your department. For example, using “WNL” instead of “within normal limits” might be unclear to non-clinical staff.
Use concise and direct sentences
Your SOAP notes should make it easy digest highlights from your patient examination quickly.
Long sentences and big walls of text will make your notes hard to scan. If you take a look at the SOAP note examples above, you’ll notice that clinicians don’t have to write in full sentences, and bullet points are used to make their notes more skimmable.
Even when notes are written in paragraph form, these sentences are straight to the point.
- DO: Write short sentences focusing on essential information, key findings, and actions.
- DON'T: Use complex descriptions and wordy sentences to describe a patient encounter. For example — “Patient reports headache that worsens in bright light” instead of “The patient described having headaches that become more painful every time they look at something bright around the house.”
Don't add excessive detail
Note bloat is real. Although adding context from patient encounters is important, you’ll also want to be mindful that the details you include are relevant to the concern you have at hand.
For example, adding information from friendly conversations with patients into your notes won’t add a clear benefit to the next step in your care plan.
Instead, it will cause clutter and make it harder to deduce essential action items. The same goes for recollections of past symptoms and medical history that aren’t relevant to the problem the patient is presenting.
- DO: Focus your notes on observations, rationales, and action related to the patient’s primary concern.
- DON'T: Include anecdotes and history unrelated to the assessment you’re trying to make. In that first SOAP note example, the patient having pasta and meatballs for dinner was important because that’s when their pain started. But you wouldn’t want to highlight what the patient watched on TV while having dinner.
Structure your SOAP notes in logical order
The SOAP structure was created to help clinicians present their findings in an organized way.
It also helps you document your observations and rationale by order of importance and relevance so that it’s easy for other healthcare providers to follow. Arranging your notes logically helps you tell your patient’s story accurately and with the right context.
- DO: Understand the requirements of each SOAP section and follow the format provided: Subjective first, followed by Objective, Assessment, and Plan.
- DON'T: Rearrange sections or blend content from different sections together.
Keep a professional and objective tone
Your clinical notes are factual documents that serve a clear purpose of helping patients get the care they need based on the concerns they’re presenting.
Your notes must remain unbiased and solely focused on the medical problem you’re trying to assess.
- DO: Use neutral language that focuses on actual observations and descriptions of the situation in front of you.
- DON'T: Make assumptions or accusations of a patient’s character or behavior based on your impression of them during an encounter. For example, a healthcare provider should not be documenting their personal opinion on unrelated lifestyle habits or health challenges.
Try a SOAP note generator that documents for you
SOAP notes across specialties
The SOAP framework adapts to every clinical context, but the emphasis shifts by discipline. Freed has dedicated guides for each:
- Physical Therapy SOAP Notes — ROM measurements, functional goals, phase-based progression
- Psychiatric SOAP Notes — mental status exam, mood/affect documentation, medication management
- Occupational Therapy SOAP Notes — ADL function, goal progress, skilled intervention documentation
- EMS SOAP Narrative — prehospital adaptations for rapid assessment
Write SOAP notes faster with Freed
Freed's AI scribe listens to your patient encounter — in person or via telehealth — and generates a complete SOAP note in your preferred format and style. Clinicians report saving 2–3 hours of documentation time per day.
Freed is HIPAA-compliant, works with EHR systems, and takes about 60 seconds to set up.
Try Freed free → No credit card required.
How to Write SOAP Notes: Real Examples + Free Template (2026)
Table of Contents
You can defuse a crisis at 10 am, soothe a patient's meltdown at 10:30, and maybe even perform a minor miracle before noon.
But having to catch up on SOAP notes after all that? Sometimes, that's the loose thread that can unravel anyone's sanity.
The SOAP format has been a staple of clinical documentation for over 50 years — but let's face it, it isn't always smooth sailing. Time crunches, juggling consistency, and figuring out what details matter most can leave even seasoned clinicians at a loss.
In this guide, you'll find real SOAP note examples across specialties, a free copy-paste template, and tips from clinicians who've cracked the code on writing notes without sacrificing their evenings.
Want the note written for you? Freed's AI scribe listens to your visit and generates a complete SOAP note in about 60 seconds. Try it free →
What are SOAP notes?
SOAP notes are the tried-and-true format most clinicians use to document patient encounters. SOAP stands for Subjective, Objective, Assessment, and Plan — four sections that organize your findings, clinical reasoning, and next steps into a format any provider can follow.
Here's why the structure matters:
- Improves efficiency: Clinicians can quickly locate key information — reported symptoms, diagnostic findings, care plan — without searching through paragraph-heavy notes. A clear structure also supports legal, billing, and audit requirements.
- Supports clinical decision-making: Separating notes into defined sections helps you present assessments and rationale logically. SOAP notes empower providers to act on clearly documented evidence.
- Enhances patient outcomes: A well-documented SOAP note creates accountability for thorough, actionable care plans. Comprehensiveness with purpose — not aimless length.
- Simplifies standardization: SOAP's consistency sets it apart from other frameworks like DAP (Data, Assessment, Plan). SOAP is precise and evidence-based; DAP is more flexible. For multidisciplinary or evidence-heavy documentation, SOAP wins.
A brief history: Why SOAP notes exist
SOAP wasn't invented by a committee. It came from one clinician who was frustrated enough to build something better.
Larry Weed was both a practicing physician and a research scientist. Standing in both worlds, he saw what medicine lacked: a systematic way to organize clinical thinking.
In his words:
"A physician works in a chaotic system of keeping and organizing data and has no systematic review and correction of his daily work."
So he built one. Weed's problem-oriented medical record, developed in the 1960s, introduced the idea that a clinical note should start with the problem in front of you — not the clinician's impression of it. He wanted data, not bias.
The result was the problem list — and eventually, the SOAP format. It took four years to rearrange how medicine documented patient care, but the framework Weed built became the backbone of modern clinical documentation.
His standard for a good note: thorough, reliable, analytically sound, and efficient. Not longer. Just better.
SOAP note format: what goes in each section
Each section of this type of progress note has a specific purpose in helping clinicians sort their findings, data, and care recommendations.
Here's a quick reference:
Let's break down each section with examples:
Subjective
The subjective section captures a patient’s subjective perspective about their concerns and experiences.
You’ll document the:
- Primary problem (chief complaint) presented in the patient encounter,
- The review of systems (ROS) to see how and if symptoms present
- Other relevant information like medical history or lifestyle habits that could be related to their complaint.
Examples of a Subjective
- Mr. Jones' chief complaint is a back pain. He also exercises 5x a week with heavy weights.
- Angie complained of abdominal pain that has persisted for the past two days.
Helpful tip
If you can't measure or verify it directly, it belongs in Subjective.
Objective
The objective section records of measurable data collected during a patient’s visit, such as physical exam results and laboratory results completed during that time. Physicians will also add their observations or direct patient quotes to this section.
Examples of an Objective
- Mr. Jones' vital signs are normal. His lower back has tenderness to palpation.
- Angie’s abdomen has no rebound tenderness in the lower right quadrant. No visible swelling or bruising.
Helpful tip
Use shorthand where appropriate, but spell out anything a provider outside your specialty might not recognize.
Assessment
This assessment section summarizes the patient’s perspectives and physician observations into a clinical diagnosis.
This section holds the most weight in your SOAP note as it describes a thorough analysis of the patient’s problems, all possible diagnoses, and the reasoning behind that diagnosis.
Examples of an Assessment
- Lower back pain is a lumbar muscle strain from overexertion during heavy weightlifting. A different diagnosis could be a Vitamin D deficiency.
- Abdominal pain without signs of acute abdomen or significant palpation. Likely gastrointestinal discomfort or mild inflammation.
Helpful tip
Don't just name the diagnosis — show the thread.
Plan
The plan section (usually combined with assessment) outlines the next steps in your recommended treatment plan. You’ll use this section to detail information such as action items for future examinations, required medication, or referrals for more testing or consultations with specialists.
Examples of a Plan
- Recommend avoidance of heavy lifting for one to two weeks. Prescribe a mild analgesic for pain and a diagnostic test for D3 deficiency. Schedule a follow-up appointment next week.
- Prescribe over-the-counter antacids for relief when needed. Monitor for symptoms like fever, severe pain, nausea, or vomiting.
Helpful tip:
In many specialties, Assessment and Plan are combined into a single A&P section for efficiency. This is accepted practice.
SOAP note examples (and what you can learn from them)
The examples below will help you better visualize how healthcare providers use the SOAP template to structure and guide their clinical documentation.
We've included both illustrated examples and fully written text examples you can learn from directly.
Example 1: SOAP note for abdominal pain (primary care)
What can we learn from this example?
- It provides a clear timeline with descriptions of symptoms, including patient quotes and relevant anecdotes for clarity.
- It includes vital signs and specific diagnostic indicators for a more precise diagnosis.
- The assessment is supported by clinical findings that differentiate possible conditions and reference relevant literature.
- The document includes clear next steps and provides actionable patient instructions.
Example 2: SOAP note chronic disease follow-up (diabetes management)
What can we learn from this example?
- The note is concise and avoids unnecessary details, making it easier for healthcare providers to understand the patient’s condition and care plan.
- The patient’s history, symptoms, and self-reported readings are documented because they are relevant to her diabetes management.
- The plan clearly describes ongoing management strategies and outlines appropriate follow-ups, and includes specific instructions for pre-visit tests, laboratory results, and diagnostic results
Get a free, downloadable SOAP note template
6 tips for writing powerful SOAP notes
Beyond understanding the purpose of each SOAP section, clinicians have to approach the note-taking process with a clear understanding of how to optimize their language choices and writing styles specifically for documentation.
Now that you've seen what strong clinical notes look like in action, let's review a few important reminders that reinforce the clarity, effectiveness, and overall efficiency of your medical notes.
Avoid jargon and abbreviations
Remember that SOAP notes aim to help your entire healthcare team ensure accuracy, drive patient care forward, and avoid miscommunication.
Using universal language that multidisciplinary healthcare providers can understand is important in making your documentation readable and easy to act on.
The next provider meeting your patient may be someone outside your specialty. If that’s the case, you’ll want to:
- Do: Explain acronyms the first time you use them if you need to bring that acronym up.
- Don’t: Use shorthand commonly used in your department. For example, using “WNL” instead of “within normal limits” might be unclear to non-clinical staff.
Use concise and direct sentences
Your SOAP notes should make it easy digest highlights from your patient examination quickly.
Long sentences and big walls of text will make your notes hard to scan. If you take a look at the SOAP note examples above, you’ll notice that clinicians don’t have to write in full sentences, and bullet points are used to make their notes more skimmable.
Even when notes are written in paragraph form, these sentences are straight to the point.
- DO: Write short sentences focusing on essential information, key findings, and actions.
- DON'T: Use complex descriptions and wordy sentences to describe a patient encounter. For example — “Patient reports headache that worsens in bright light” instead of “The patient described having headaches that become more painful every time they look at something bright around the house.”
Don't add excessive detail
Note bloat is real. Although adding context from patient encounters is important, you’ll also want to be mindful that the details you include are relevant to the concern you have at hand.
For example, adding information from friendly conversations with patients into your notes won’t add a clear benefit to the next step in your care plan.
Instead, it will cause clutter and make it harder to deduce essential action items. The same goes for recollections of past symptoms and medical history that aren’t relevant to the problem the patient is presenting.
- DO: Focus your notes on observations, rationales, and action related to the patient’s primary concern.
- DON'T: Include anecdotes and history unrelated to the assessment you’re trying to make. In that first SOAP note example, the patient having pasta and meatballs for dinner was important because that’s when their pain started. But you wouldn’t want to highlight what the patient watched on TV while having dinner.
Structure your SOAP notes in logical order
The SOAP structure was created to help clinicians present their findings in an organized way.
It also helps you document your observations and rationale by order of importance and relevance so that it’s easy for other healthcare providers to follow. Arranging your notes logically helps you tell your patient’s story accurately and with the right context.
- DO: Understand the requirements of each SOAP section and follow the format provided: Subjective first, followed by Objective, Assessment, and Plan.
- DON'T: Rearrange sections or blend content from different sections together.
Keep a professional and objective tone
Your clinical notes are factual documents that serve a clear purpose of helping patients get the care they need based on the concerns they’re presenting.
Your notes must remain unbiased and solely focused on the medical problem you’re trying to assess.
- DO: Use neutral language that focuses on actual observations and descriptions of the situation in front of you.
- DON'T: Make assumptions or accusations of a patient’s character or behavior based on your impression of them during an encounter. For example, a healthcare provider should not be documenting their personal opinion on unrelated lifestyle habits or health challenges.
Try a SOAP note generator that documents for you
SOAP notes across specialties
The SOAP framework adapts to every clinical context, but the emphasis shifts by discipline. Freed has dedicated guides for each:
- Physical Therapy SOAP Notes — ROM measurements, functional goals, phase-based progression
- Psychiatric SOAP Notes — mental status exam, mood/affect documentation, medication management
- Occupational Therapy SOAP Notes — ADL function, goal progress, skilled intervention documentation
- EMS SOAP Narrative — prehospital adaptations for rapid assessment
Write SOAP notes faster with Freed
Freed's AI scribe listens to your patient encounter — in person or via telehealth — and generates a complete SOAP note in your preferred format and style. Clinicians report saving 2–3 hours of documentation time per day.
Freed is HIPAA-compliant, works with EHR systems, and takes about 60 seconds to set up.
Try Freed free → No credit card required.
FAQs
Frequently asked questions from clinicians and medical practitioners.
What are SOAP notes?
What does SOAP stand for in notes?
What is an example of a SOAP note for OT?
How do I write a physical therapy SOAP note?
What’s the difference between SOAP, DAP, and other progress note formats?
How do I generate effective SOAP notes?
Who uses SOAP notes?
How long should a SOAP note be?
How does Freed generate SOAP notes?
.avif)
Related content
Free yourself for better things
548 Market Street, PMB 95301
San Francisco, CA 94104
Specialties
Compliance & Security
Our technology is HIPAA-compliant, uses industry best practices, and doesn’t store patient recordings.