Occupational Therapy SOAP Notes [+ Free Template]
Four sessions in. One patient is finally showing improved independence in activities of daily living, another is struggling with dressing again, and your next therapy session is already starting.
You remember fragments of the first therapy session, but not enough to confidently write accurate clinical documentation.
This is where the SOAP note becomes essential.
“SOAP notes can be tricky because we occupational therapists (OTs) are so detail-oriented." — Janis Galindez, occupational therapist
For healthcare professionals, especially in occupational therapy, the SOAP note format is not just paperwork. It's a standardized method for capturing patient care, ensuring continuity of care, and documenting patient progress in a structured format.
But when documentation piles up, even experienced clinicians struggle to maintain consistent SOAP note quality.
This guide breaks down everything you need to know about occupational therapy SOAP notes, including structure, examples, and how to improve clinical efficiency using a standardized method of documentation.
What is an occupational therapy SOAP note?
SOAP notes use a structured format used in clinical documentation to record patient care during a therapy session. It is widely used across healthcare systems as a communication tool between healthcare providers.
In occupational therapy, a SOAP note helps clinicians document:
- Subjective information from the patient
- Objective measurable data from the session
- Assessment using clinical reasoning
- Plan for ongoing treatment
This SOAP note format ensures consistent documentation, supports medical records, and improves continuity of care across providers.
For occupational therapy, this structured method ensures that every patient’s condition is accurately reflected in clinical documentation.
In busy clinical settings, having this type of note capture a treatment plan helps therapists get clarity in their work.
Free occupational therapy SOAP note template
Don’t want to start from scratch? Here’s a plug-and-play template to keep your notes focused and functional.
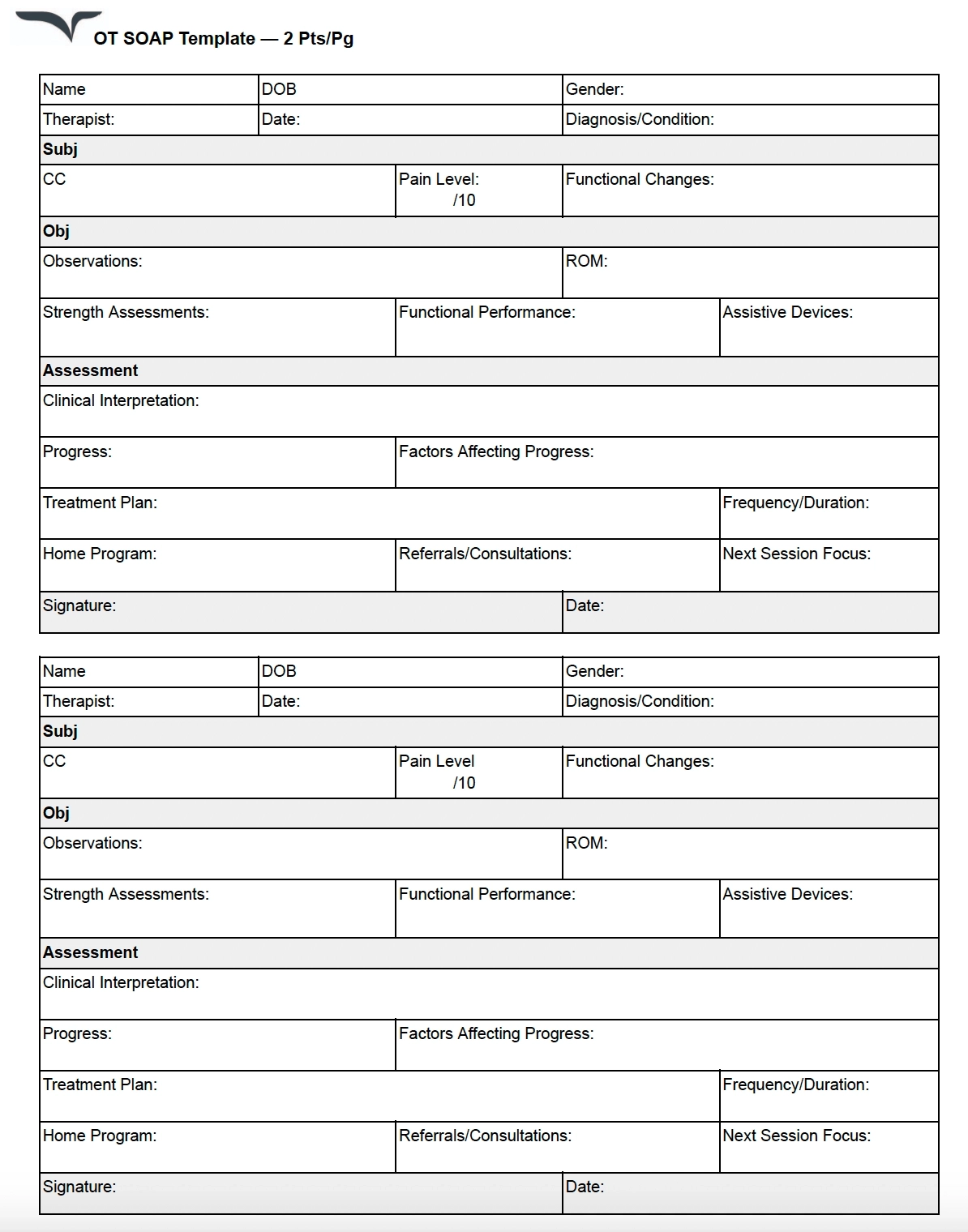
The SOAP note format for occupational therapy
SOAP stands for Subjective, Objective, Assessment, and Plan. Each section plays a critical role in therapy documentation, clinical reasoning, and communication between healthcare providers. Let’s break down what each section would look like if you’re an OT, occupational therapist assistant (OTA), or OT student.
SUBJECTIVE (Patient-reported information)
The subjective section captures the patient’s condition from their perspective. The subjective section includes subjective data, such as:
- Chief complaint
- Reported pain or discomfort
- Emotional or cognitive concerns
- Patient-reported limitations in activities of daily living
Example subjective statements in a SOAP note:
- “Patient reports difficulty with self-care tasks in the morning.”
- “Patient states increased fatigue during daily activities.”
- “Caregiver reports changes in patient independence at home.”
The subjective section is critical for understanding the patient’s lived experience.
In occupational therapy, subjective data helps guide clinical reasoning and supports development of a treatment plan. The subjective section in a SOAP note is often the foundation for identifying goals in occupational therapy.
OBJECTIVE (Measurable and observable data)
The objective section contains measurable data and observable data collected during the therapy session.
The objective section includes:
- Range of motion measurements
- Strength testing
- Task performance
- Functional performance in ADLs
- Clinical observations
Example objective documentation:
- Patient completed grooming task with 70% independence
- Patient demonstrated improved grip strength
- Patient required minimal assistance during dressing
The objective section provides objective data that supports clinical reasoning. In occupational therapy, the objective section is essential for evaluating patient progress and treatment effectiveness. Accurate objective data improves clinical documentation and ensures consistency in medical records.
ASSESSMENT (Clinical interpretation)
The assessment section is where clinical reasoning is applied.
In the assessment, clinicians interpret subjective data and objective data to determine:
- Progress toward treatment goals
- Barriers to functional goals
- Changes in patient outcomes
- Effectiveness of interventions
The assessment is not just a summary—it is professional judgment.
Example assessment:
- Patient shows improved functional performance but continues to require assistance in ADLs.
- Patient demonstrates moderate progress toward treatment goals with improved upper extremity strength.
- Patient’s condition indicates ongoing need for skilled occupational therapy.
The assessment section is central to the SOAP note format, as it reflects clinical reasoning in occupational therapy.
A strong assessment improves communication between healthcare professionals and supports continuity of care.
PLAN (Next steps in treatment)
The plan outlines the next steps in care.
The plan may include:
- Upcoming therapy session goals
- Updates to treatment plan
- Home exercises
- Caregiver education
- Adjustments to therapeutic activities
Example plan:
- Continue occupational therapy focusing on ADLs
- Introduce new therapeutic activities to improve functional performance
- Update treatment plan based on patient progress
- Monitor treatment effectiveness in next session
The plan ensures structured follow-up and continuity of care. Each plan contributes to ongoing patient care and supports long-term patient outcomes.
OT SOAP note examples (6 real-world settings)
Example 1: Adult rehabilitation
Subjective: Patient reports difficulty completing activities of daily living and increased fatigue.
Objective: Patient completed dressing task with moderate assistance and demonstrated improved observable data in upper extremity movement.
Assessment: Patient shows gradual improvement in functional performance, but continues to require assistance in ADLs.
Plan: Continue treatment plan focusing on independence in daily activities.
Example 2: Pediatric occupational therapy
Subjective: Patient reports frustration with handwriting during school tasks.
Objective: Patient demonstrated improved measurable data in fine motor control during therapy session.
Assessment: Patient shows progress in functional goals but continues to require support.
Plan: Continue therapeutic activities targeting handwriting and ADLs.
Example 3: Pediatric sensory processing
Subjective: Parent reports child has been refusing to wear clothing with tags and melting down during morning dressing routines daily this week.
Objective: Client participated in a 45-minute sensory integration session. Tolerated brushing protocol on upper extremities for 3 minutes with minimal verbal protest (compared to refusal in previous session). Engaged in proprioceptive activities (wall push-ups, weighted blanket) for 10 minutes with sustained attention.
Assessment: Client demonstrates tactile hypersensitivity consistent with sensory processing challenges impacting ADL independence and family routines. Improved tolerance to tactile input observed this session, suggesting responsiveness to sensory diet interventions.
Plan: Continue sensory integration protocol twice weekly. Educate caregiver on sensory diet strategies for morning routine. Introduce tag-free clothing trial as home program goal.
Example 4: Inpatient/SNF — Upper extremity post-stroke
Subjective: Patient reports increased frustration with inability to button shirt independently. States, "My right hand just won't cooperate."
Objective: Patient engaged in 30-minute OT session targeting right upper extremity fine motor function. Completed 5/10 button trials independently with verbal cueing. Active range of motion: shoulder flexion 0–95°, elbow extension 0–10° deficit. Grip strength measured at 12 lbs right, 38 lbs left.
Assessment: Patient demonstrates moderate deficits in right UE fine motor function and grip strength secondary to CVA, limiting independence in instrumental ADLs. Motivation and verbal engagement indicate strong rehabilitation potential.
Plan: Continue OT 5x/week. Progress button trials to clothing with varied fastener types. Introduce adaptive button hook. Reassess grip strength at next session.
Example 5: Mental health/psychiatric OT
Subjective: Client reports difficulty maintaining a daily routine since discharge. States they "can't seem to get out of bed before noon."
Objective: Client participated in a 50-minute occupational therapy session focused on daily living skills and routine building. Completed a morning routine simulation (hygiene, meal prep, medication management) with moderate verbal cueing. Identified two personal goals related to employment.
Assessment: Client demonstrates functional deficits in executive function and task initiation impacting ability to maintain a structured daily routine. Goal-setting engagement indicates readiness to work toward community reintegration.
Plan: Develop personalized daily routine schedule with client. Introduce habit-stacking strategies. Coordinate with treatment team regarding vocational rehabilitation referral.
Example 6: A functional kitchen assessment
Here’s a real-world SOAP note example shared on Reddit by an occupational therapist. This particular note captures a functional kitchen assessment with an adult patient.
Subjective: OT introduced self and explained the role. Verbal consent was obtained to complete a functional kitchen assessment.
Objective: Patient was seated upon arrival and performed an independent sit-to-stand transfer. Mobilized approximately 10 meters to the kitchen using a wheeled Zimmer frame (wzf). Initiated task by filling and plugging in the kettle. Located a mug, spoon, milk, and teabags with minimal supervision. Added the teabag to the mug, safely poured boiling water, added milk, and removed the teabag using the spoon. Patient then mobilized back to bedside with wzf.
Assessment: Patient demonstrated independent mobility with the use of a wzf and required no assistance with chair transfers. Successfully planned and sequenced the task of making a hot drink, indicating functional cognitive and physical abilities.
Plan: No further OT input required. Discharge from occupational therapy services.
The benefits of SOAP notes for OTs
When done right, SOAP notes are more than just a documentation requirement. They keep OTs sane and ready to tackle a day of juggling multiple patient interactions while ensuring the best plan of care is documented with accuracy.
“As a pediatric OT you see so many clients and families, prepare for sessions, work on reports, and so much more that it is so easy to forget what you did with your kid in the last session,” says Galindez.
Here are a few reasons why Galindez uses the SOAP note as a preferred type of note:
- Jog your memory: When you’re juggling multiple clients and sessions, SOAP notes make it easier to recall what interventions you used and how a client responded, without relying on memory alone.
- Improve collaboration: Well-written notes help you communicate clearly with families, teachers, and other providers, keeping everyone on the same page about a client’s progress.
- Speed up with practice: Build your system, reuse smart blurbs, and suddenly notes aren’t the time suck they used to be.
For healthcare professionals, the SOAP note format is a standardized method that ensures clarity in medical records.It also strengthens documentation across therapy sessions and improves patient outcomes.
Writing effective OT SOAP notes
Having good best practices and processes handy ensures that notetaking adds value and not unwanted effort into your workflow.
“I see about seven kids per day, so writing SOAP notes can be overwhelming, especially when I am seeing kids back to back,” Galindez shares.
Here are a few more of her go-to strategies for managing SOAP notes without burning out:
- Take advantage of built-in breaks. If your schedule includes a few minutes after each session, use that time to jot down notes while the session is still fresh in your mind.
- Speak up about your workload. If you’re a student or new grad, don’t be afraid to advocate for protected documentation time. You’re advocating for yourself and the best care for your clients.
- Explore in-session documentation (when appropriate). If it doesn’t interfere with your connection to the client, taking brief notes during a session can help reduce the backlog at the end of the day.
Here are some other tips to remember:
SOAP notes and clinical efficiency
For occupational therapy, SOAP notes are a communication tool that supports clinical workflow.
They improve:
- Therapy documentation efficiency
- Patient outcomes tracking
- Treatment effectiveness evaluation
- Healthcare provider communication
A consistent SOAP note system reduces cognitive load during busy therapy sessions and improves overall patient care.
Galindez’s biggest tip? Advocate for your time.
“I’m allotted a couple of minutes after each session for documentation, but I know this isn’t the case at every clinic. I always urge new students and graduates to advocate for their time because having that is important for providing the best care.”
With a few smart tips, a reusable structure, and supporting tools that speak your language, your notes can stop being the end-of-day headache — and actually help.
How Freed helps OTs write SOAP notes faster
Freed listens to your session in the background and generates a structured SOAP note automatically — Subjective, Objective, Assessment, and Plan — ready for your review when the session ends.
For OTs seeing six or seven clients a day, that means no more catching up on notes during your lunch break or at 9pm. You review, edit if needed, and sign off. Freed learns your preferences over time, adapting to your documentation style and the functional language you use most.
Turn your existing patient intake forms into reusable templates. Simply upload a note, and Freed evaluates its structure, formatting, and content to create a template you can apply to future visits. You can also select from Freed’s extensive template library. As you continue editing notes, Freed adapts and refines your templates automatically to better match your workflow.
Freed is HIPAA-compliant and built for clinical workflows — including occupational therapy, physical therapy, speech therapy, and behavioral health.
Ready to make SOAP notes work for you?
Want to skip the mental load and still get perfect notes? Try Freed's AI scribe.
Disclaimer: This article is for informational purposes only and does not constitute legal or clinical advice. Clinicians should follow applicable laws, regulations, and institutional policies when creating or sharing occupational therapy SOAP notes.
Table of Contents
Four sessions in. One patient is finally showing improved independence in activities of daily living, another is struggling with dressing again, and your next therapy session is already starting.
You remember fragments of the first therapy session, but not enough to confidently write accurate clinical documentation.
This is where the SOAP note becomes essential.
“SOAP notes can be tricky because we occupational therapists (OTs) are so detail-oriented." — Janis Galindez, occupational therapist
For healthcare professionals, especially in occupational therapy, the SOAP note format is not just paperwork. It's a standardized method for capturing patient care, ensuring continuity of care, and documenting patient progress in a structured format.
But when documentation piles up, even experienced clinicians struggle to maintain consistent SOAP note quality.
This guide breaks down everything you need to know about occupational therapy SOAP notes, including structure, examples, and how to improve clinical efficiency using a standardized method of documentation.
What is an occupational therapy SOAP note?
SOAP notes use a structured format used in clinical documentation to record patient care during a therapy session. It is widely used across healthcare systems as a communication tool between healthcare providers.
In occupational therapy, a SOAP note helps clinicians document:
- Subjective information from the patient
- Objective measurable data from the session
- Assessment using clinical reasoning
- Plan for ongoing treatment
This SOAP note format ensures consistent documentation, supports medical records, and improves continuity of care across providers.
For occupational therapy, this structured method ensures that every patient’s condition is accurately reflected in clinical documentation.
In busy clinical settings, having this type of note capture a treatment plan helps therapists get clarity in their work.
Free occupational therapy SOAP note template
Don’t want to start from scratch? Here’s a plug-and-play template to keep your notes focused and functional.
The SOAP note format for occupational therapy
SOAP stands for Subjective, Objective, Assessment, and Plan. Each section plays a critical role in therapy documentation, clinical reasoning, and communication between healthcare providers. Let’s break down what each section would look like if you’re an OT, occupational therapist assistant (OTA), or OT student.
SUBJECTIVE (Patient-reported information)
The subjective section captures the patient’s condition from their perspective. The subjective section includes subjective data, such as:
- Chief complaint
- Reported pain or discomfort
- Emotional or cognitive concerns
- Patient-reported limitations in activities of daily living
Example subjective statements in a SOAP note:
- “Patient reports difficulty with self-care tasks in the morning.”
- “Patient states increased fatigue during daily activities.”
- “Caregiver reports changes in patient independence at home.”
The subjective section is critical for understanding the patient’s lived experience.
In occupational therapy, subjective data helps guide clinical reasoning and supports development of a treatment plan. The subjective section in a SOAP note is often the foundation for identifying goals in occupational therapy.
OBJECTIVE (Measurable and observable data)
The objective section contains measurable data and observable data collected during the therapy session.
The objective section includes:
- Range of motion measurements
- Strength testing
- Task performance
- Functional performance in ADLs
- Clinical observations
Example objective documentation:
- Patient completed grooming task with 70% independence
- Patient demonstrated improved grip strength
- Patient required minimal assistance during dressing
The objective section provides objective data that supports clinical reasoning. In occupational therapy, the objective section is essential for evaluating patient progress and treatment effectiveness. Accurate objective data improves clinical documentation and ensures consistency in medical records.
ASSESSMENT (Clinical interpretation)
The assessment section is where clinical reasoning is applied.
In the assessment, clinicians interpret subjective data and objective data to determine:
- Progress toward treatment goals
- Barriers to functional goals
- Changes in patient outcomes
- Effectiveness of interventions
The assessment is not just a summary—it is professional judgment.
Example assessment:
- Patient shows improved functional performance but continues to require assistance in ADLs.
- Patient demonstrates moderate progress toward treatment goals with improved upper extremity strength.
- Patient’s condition indicates ongoing need for skilled occupational therapy.
The assessment section is central to the SOAP note format, as it reflects clinical reasoning in occupational therapy.
A strong assessment improves communication between healthcare professionals and supports continuity of care.
PLAN (Next steps in treatment)
The plan outlines the next steps in care.
The plan may include:
- Upcoming therapy session goals
- Updates to treatment plan
- Home exercises
- Caregiver education
- Adjustments to therapeutic activities
Example plan:
- Continue occupational therapy focusing on ADLs
- Introduce new therapeutic activities to improve functional performance
- Update treatment plan based on patient progress
- Monitor treatment effectiveness in next session
The plan ensures structured follow-up and continuity of care. Each plan contributes to ongoing patient care and supports long-term patient outcomes.
OT SOAP note examples (6 real-world settings)
Example 1: Adult rehabilitation
Subjective: Patient reports difficulty completing activities of daily living and increased fatigue.
Objective: Patient completed dressing task with moderate assistance and demonstrated improved observable data in upper extremity movement.
Assessment: Patient shows gradual improvement in functional performance, but continues to require assistance in ADLs.
Plan: Continue treatment plan focusing on independence in daily activities.
Example 2: Pediatric occupational therapy
Subjective: Patient reports frustration with handwriting during school tasks.
Objective: Patient demonstrated improved measurable data in fine motor control during therapy session.
Assessment: Patient shows progress in functional goals but continues to require support.
Plan: Continue therapeutic activities targeting handwriting and ADLs.
Example 3: Pediatric sensory processing
Subjective: Parent reports child has been refusing to wear clothing with tags and melting down during morning dressing routines daily this week.
Objective: Client participated in a 45-minute sensory integration session. Tolerated brushing protocol on upper extremities for 3 minutes with minimal verbal protest (compared to refusal in previous session). Engaged in proprioceptive activities (wall push-ups, weighted blanket) for 10 minutes with sustained attention.
Assessment: Client demonstrates tactile hypersensitivity consistent with sensory processing challenges impacting ADL independence and family routines. Improved tolerance to tactile input observed this session, suggesting responsiveness to sensory diet interventions.
Plan: Continue sensory integration protocol twice weekly. Educate caregiver on sensory diet strategies for morning routine. Introduce tag-free clothing trial as home program goal.
Example 4: Inpatient/SNF — Upper extremity post-stroke
Subjective: Patient reports increased frustration with inability to button shirt independently. States, "My right hand just won't cooperate."
Objective: Patient engaged in 30-minute OT session targeting right upper extremity fine motor function. Completed 5/10 button trials independently with verbal cueing. Active range of motion: shoulder flexion 0–95°, elbow extension 0–10° deficit. Grip strength measured at 12 lbs right, 38 lbs left.
Assessment: Patient demonstrates moderate deficits in right UE fine motor function and grip strength secondary to CVA, limiting independence in instrumental ADLs. Motivation and verbal engagement indicate strong rehabilitation potential.
Plan: Continue OT 5x/week. Progress button trials to clothing with varied fastener types. Introduce adaptive button hook. Reassess grip strength at next session.
Example 5: Mental health/psychiatric OT
Subjective: Client reports difficulty maintaining a daily routine since discharge. States they "can't seem to get out of bed before noon."
Objective: Client participated in a 50-minute occupational therapy session focused on daily living skills and routine building. Completed a morning routine simulation (hygiene, meal prep, medication management) with moderate verbal cueing. Identified two personal goals related to employment.
Assessment: Client demonstrates functional deficits in executive function and task initiation impacting ability to maintain a structured daily routine. Goal-setting engagement indicates readiness to work toward community reintegration.
Plan: Develop personalized daily routine schedule with client. Introduce habit-stacking strategies. Coordinate with treatment team regarding vocational rehabilitation referral.
Example 6: A functional kitchen assessment
Here’s a real-world SOAP note example shared on Reddit by an occupational therapist. This particular note captures a functional kitchen assessment with an adult patient.
Subjective: OT introduced self and explained the role. Verbal consent was obtained to complete a functional kitchen assessment.
Objective: Patient was seated upon arrival and performed an independent sit-to-stand transfer. Mobilized approximately 10 meters to the kitchen using a wheeled Zimmer frame (wzf). Initiated task by filling and plugging in the kettle. Located a mug, spoon, milk, and teabags with minimal supervision. Added the teabag to the mug, safely poured boiling water, added milk, and removed the teabag using the spoon. Patient then mobilized back to bedside with wzf.
Assessment: Patient demonstrated independent mobility with the use of a wzf and required no assistance with chair transfers. Successfully planned and sequenced the task of making a hot drink, indicating functional cognitive and physical abilities.
Plan: No further OT input required. Discharge from occupational therapy services.
The benefits of SOAP notes for OTs
When done right, SOAP notes are more than just a documentation requirement. They keep OTs sane and ready to tackle a day of juggling multiple patient interactions while ensuring the best plan of care is documented with accuracy.
“As a pediatric OT you see so many clients and families, prepare for sessions, work on reports, and so much more that it is so easy to forget what you did with your kid in the last session,” says Galindez.
Here are a few reasons why Galindez uses the SOAP note as a preferred type of note:
- Jog your memory: When you’re juggling multiple clients and sessions, SOAP notes make it easier to recall what interventions you used and how a client responded, without relying on memory alone.
- Improve collaboration: Well-written notes help you communicate clearly with families, teachers, and other providers, keeping everyone on the same page about a client’s progress.
- Speed up with practice: Build your system, reuse smart blurbs, and suddenly notes aren’t the time suck they used to be.
For healthcare professionals, the SOAP note format is a standardized method that ensures clarity in medical records.It also strengthens documentation across therapy sessions and improves patient outcomes.
Writing effective OT SOAP notes
Having good best practices and processes handy ensures that notetaking adds value and not unwanted effort into your workflow.
“I see about seven kids per day, so writing SOAP notes can be overwhelming, especially when I am seeing kids back to back,” Galindez shares.
Here are a few more of her go-to strategies for managing SOAP notes without burning out:
- Take advantage of built-in breaks. If your schedule includes a few minutes after each session, use that time to jot down notes while the session is still fresh in your mind.
- Speak up about your workload. If you’re a student or new grad, don’t be afraid to advocate for protected documentation time. You’re advocating for yourself and the best care for your clients.
- Explore in-session documentation (when appropriate). If it doesn’t interfere with your connection to the client, taking brief notes during a session can help reduce the backlog at the end of the day.
Here are some other tips to remember:
SOAP notes and clinical efficiency
For occupational therapy, SOAP notes are a communication tool that supports clinical workflow.
They improve:
- Therapy documentation efficiency
- Patient outcomes tracking
- Treatment effectiveness evaluation
- Healthcare provider communication
A consistent SOAP note system reduces cognitive load during busy therapy sessions and improves overall patient care.
Galindez’s biggest tip? Advocate for your time.
“I’m allotted a couple of minutes after each session for documentation, but I know this isn’t the case at every clinic. I always urge new students and graduates to advocate for their time because having that is important for providing the best care.”
With a few smart tips, a reusable structure, and supporting tools that speak your language, your notes can stop being the end-of-day headache — and actually help.
How Freed helps OTs write SOAP notes faster
Freed listens to your session in the background and generates a structured SOAP note automatically — Subjective, Objective, Assessment, and Plan — ready for your review when the session ends.
For OTs seeing six or seven clients a day, that means no more catching up on notes during your lunch break or at 9pm. You review, edit if needed, and sign off. Freed learns your preferences over time, adapting to your documentation style and the functional language you use most.
Turn your existing patient intake forms into reusable templates. Simply upload a note, and Freed evaluates its structure, formatting, and content to create a template you can apply to future visits. You can also select from Freed’s extensive template library. As you continue editing notes, Freed adapts and refines your templates automatically to better match your workflow.
Freed is HIPAA-compliant and built for clinical workflows — including occupational therapy, physical therapy, speech therapy, and behavioral health.
Ready to make SOAP notes work for you?
Want to skip the mental load and still get perfect notes? Try Freed's AI scribe.
Disclaimer: This article is for informational purposes only and does not constitute legal or clinical advice. Clinicians should follow applicable laws, regulations, and institutional policies when creating or sharing occupational therapy SOAP notes.
FAQs
Frequently asked questions from clinicians and medical practitioners.
What is an example of a SOAP note for OT?
What is the difference between an OT SOAP note and a discharge note?
How can I write an occupational therapy discharge note?
What does SOAP stand for in occupational therapy?
How long should an occupational therapy SOAP note be?
What is the difference between a SOAP note and a DAP note in OT?
Do occupational therapists use SOAP notes?
Can AI write occupational therapy SOAP notes?
.avif)
Related content
Free yourself for better things
548 Market Street, PMB 95301
San Francisco, CA 94104
Specialties
Compliance & Security
Our technology is HIPAA-compliant, uses industry best practices, and doesn’t store patient recordings.