SOAP Narrative EMS Guidelines, Samples, & Tools
In emergency medicine, every second counts. You're juggling critical patients, making split-second decisions, and moving fast.
There isn’t time to stop and document it all.
We’ve put together these SOAP report guidelines to help you write faster, clearer ED notes. Whether you’re working through a high-speed trauma case or a complex cardiac event, the right approach to documentation keeps your team informed and your patients safe.
Let’s break it down.
What is a SOAP narrative in EMS?
You're in the EMS— time is of the essence. You probably already have a love-hate relationship with SOAP notes.
SOAP stands for:
- Subjective: The patient’s history, symptoms, and reported concerns.
- Objective: Measurable data, including:
- Vital signs
- Lab results
- Physical exam findings
- Assessment and Plan: The clinician’s analysis of the patient’s condition and next steps for treatment or management.
SOAP notes might not be your favorite task, but they’re the glue that keeps EMS teams on the same page — even in the middle of chaos.
Don't believe me?
Check out these use cases below.
SOAP method: examples in emergency medical services
In an EMS environment, SOAP notes can bring order to the chaos. Here are some key examples:
1. EMS SOAP narrative example: Motor vehicle collision (MVC) patient
Traffic accidents are common casualties faced in the ED. Here's a sample SOAP note:
Subjective
- Patient is a 30-year-old female who arrived via ambulance after a rear-end collision.
- Reports severe neck pain and a throbbing headache since the accident.
- Denies loss of consciousness but complains of mild dizziness and nausea.
- Medical history: No known chronic conditions; no current medications.
Objective
- Vital Signs: BP 132/80 mmHg, HR 98 bpm, RR 18 breaths/min, SpO₂ 98%.
- Physical Exam:
- General: Appears alert, in moderate distress due to pain.
- Neck: Tenderness along the cervical spine, limited range of motion due to pain.
- Neuro: Cranial nerves grossly intact; no focal deficits. Normal pupil reaction.
- Skin: No significant lacerations, minor abrasions on forearm.
- Imaging: Cervical spine X-ray pending.
- Labs: Basic metabolic panel and FBC ordered; no critical abnormalities noted so far.
Assessment
- MVA (motor vehicle accident)
- Cervical strain (whiplash); no immediate evidence of fracture or intracranial injury based on initial exam.
Plan
- Continue cervical spine precautions until imaging definitively rules out fractures.
- Administer NSAIDs (e.g., ibuprofen) or acetaminophen for pain relief, considering muscle relaxants if needed.
- Observe for signs of neurological changes or increased intracranial pressure (ICP).
- If imaging is clear and patient remains stable, consider discharge with neck support and outpatient follow-up instructions.
- Counsel patient on red-flag symptoms (worsening headache, vomiting, confusion) that warrant immediate return.
2. EMS SOAP narrative example: Chest pain/possible cardiac event
Another common complaint found in the ED is the possible chest pain scenario. Here's a sample:
Subjective
- 58-year-old male presents with central, pressure-like chest pain radiating to the left arm and jaw for approximately 45 minutes.
- Reports feeling anxious, diaphoretic, and slightly nauseous.
- Past medical history: Hypertension, hyperlipidemia. Family history of coronary artery disease.
- Medications: Takes atorvastatin and lisinopril regularly.
Objective
- Vital Signs: BP 148/92 mmHg, HR 110 bpm (tachycardic), RR 20 breaths/min, SpO₂ 97% on room air.
- Physical Exam:
- General: Pale, diaphoretic, mildly anxious.
- Cardiac: Tachycardic, no significant murmurs.
- Lungs: Clear bilaterally.
- EKG: ST-segment depressions in leads II, III, and aVF (suggestive of possible ischemia).
- Labs: Cardiac enzymes (troponin) drawn; first set pending. Electrolytes within normal limits.
Assessment
- Non-ST-Elevation Acute Coronary Syndrome (NSTE-ACS) or unstable angina.
- Patient’s risk factors and EKG changes warrant urgent cardiac evaluation.
Plan
- Start IV access, place on continuous cardiac monitoring.
- Administer aspirin (chewable) if no contraindications.
- Initiate sublingual nitroglycerin if BP remains stable, and consider morphine for pain control if needed.
- Repeat EKG in 15-30 minutes.
- Consult cardiology for possible stress test or urgent catheterization based on troponin trends and patient stability.
3. EMS SOAP narrative example: Diabetic emergency (hypoglycemia)
Now, let's look at a common case of hypoglycemia.
Subjective
- 45-year-old female with Type 1 diabetes mellitus arrives confused and diaphoretic.
- Colleague states the patient was found disoriented at work, unable to recall last insulin dose or meal.
- Past medical history: Type 1 diabetes since age 15, no known diabetic complications reported.
Objective
- Vital Signs: BP 120/70 mmHg, HR 100 bpm, RR 16 breaths/min, SpO₂ 98% on room air.
- Fingerstick Glucose: 42 mg/dL (indicating hypoglycemia).
- Exam: Patient is responsive but oriented only to person, tremulous, sweaty.
- Labs: Stat BMP shows no other acute abnormalities, but awaiting additional results to rule out electrolyte imbalances.
Assessment
- Acute symptomatic hypoglycemia likely due to insulin dosing mismatch and/or inadequate dietary intake.
Plan
- Administer 25 g of 50% dextrose (D50W) IV push; recheck blood glucose in 15 minutes.
- Monitor patient’s mental status and vitals closely; initiate IV fluids if needed.
- Once stabilized, assess patient’s home insulin regimen and dietary habits; involve diabetes educator as needed.
- Consider admission if there are concerns about the patient’s ability to manage insulin dosing or social support.
These samples show one thing: organization is everything in an emergency situation.
SOAP report guidelines for EMS
In the EMS, there's no time for note bloat. Keep your progress notes clear, concise, and actionable.
Here’s how to make them work for you:
1. Keep it brief, but complete
- Focus on vital information — skip unnecessary background info.
- Use short, direct sentences to make the note easy to scan.
Example: Instead of "The patient states that they started experiencing severe chest pain about 45 minutes ago, which has been getting progressively worse," try "45M with 45 min of worsening chest pain."
2. Prioritize critical information
- In high-acuity cases, lead with the most urgent details (e.g., unstable vitals, airway concerns).
- If needed, supplement with a secondary patient care report when more time allows.
3. Use a template or EMS note-taking tool
- A structured SOAP note template keeps things efficient and consistent.
- Use the standardized format and time-saving structure to focus on key details without extra fluff.
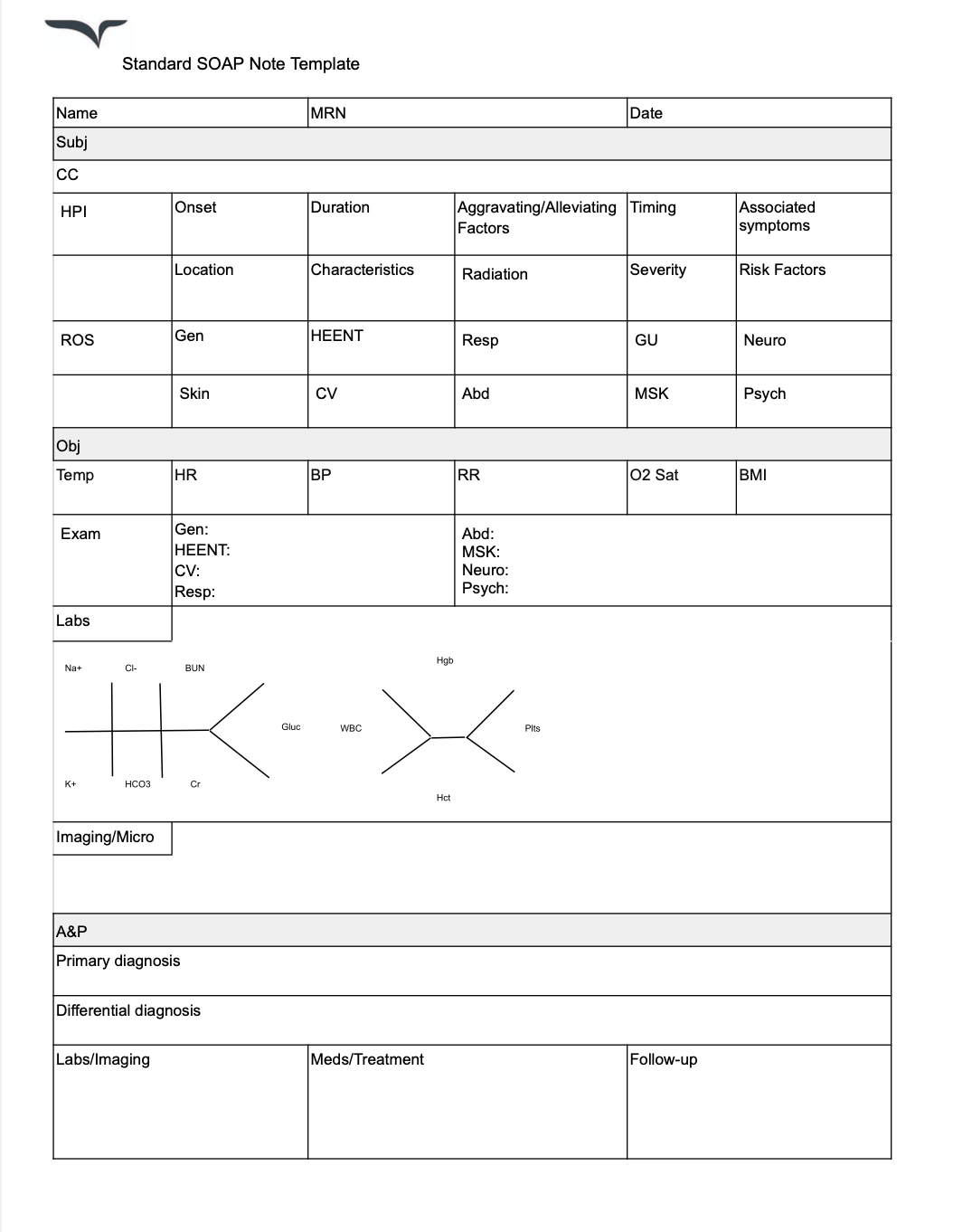
Grab your free SOAP note template here.
4. Use standardized abbreviations
- EMS teams rely on quick, universal shorthand (e.g., SOB for shortness of breath, c/o for complaints of).
- Avoid uncommon abbreviations that could cause confusion. It's not time to reinvent the wheel.
“I make use of shorthand and common medical abbreviations. These cutbacks on words not only quicken the process of documentation but also ensure clarity in the notes.” — Dr. Sam Singh; Winit Clinic
5. Be objective and neutral
- Stick to facts and observable signs rather than assumptions.
- Instead of “patient seems intoxicated,” write “slurred speech, unsteady gait, strong odor of alcohol on breath.”
6. Ensure continuity of care
- Your SOAP note should set up the next clinician for success — whether in the ED or another facility.
- Include treatment provided, patient response, and next steps to avoid redundancy or miscommunication.
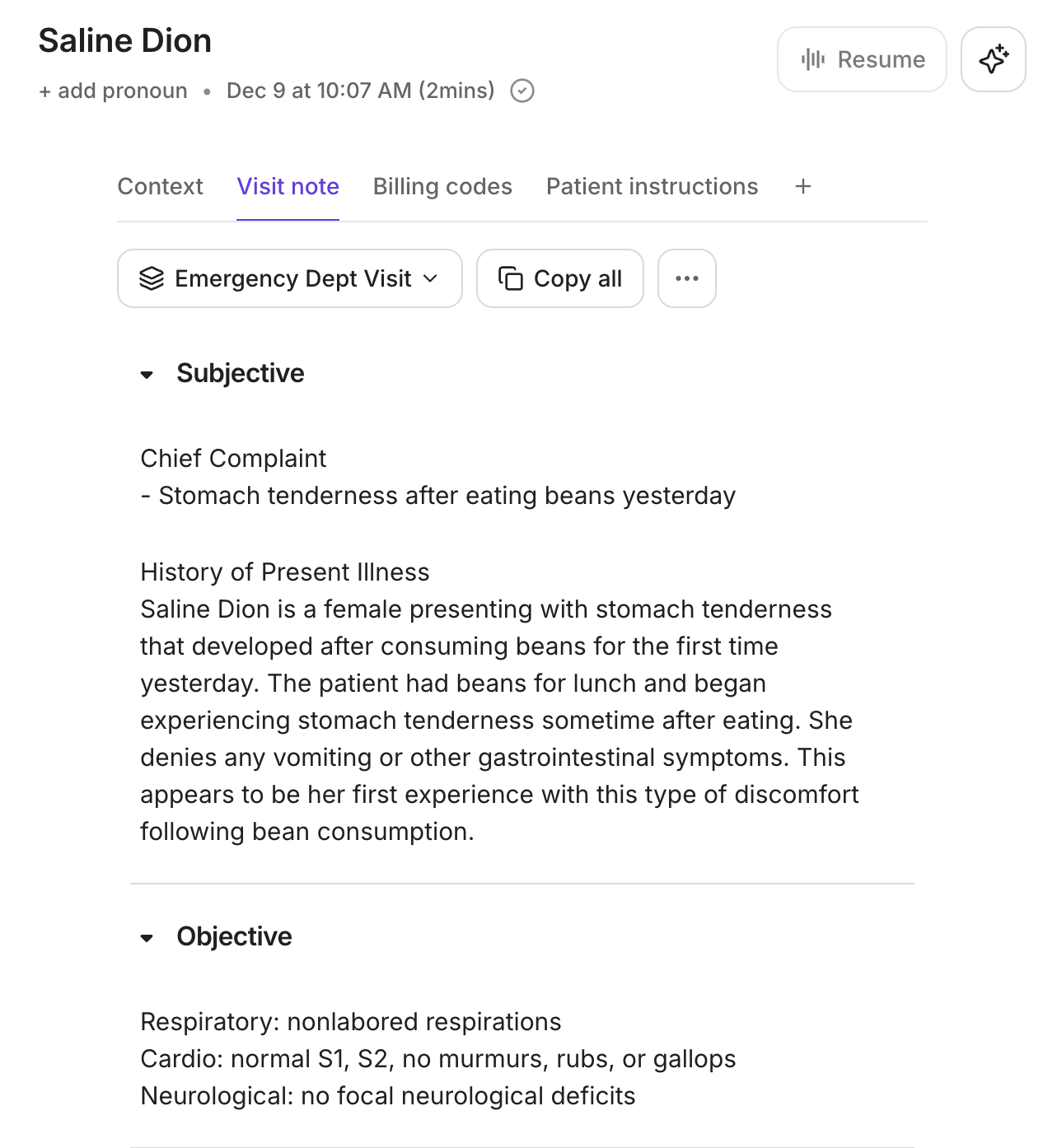
How Freed helps EMS providers document faster
AI scribes take medical dictation to the next level.
These hands-free note-taking tools are able to listen and process a conversation, turning your patient encounter into a finished medical note.
📌See how AI scribes work in ED
Benefits of using AI in EMS patient care
Multiple patients are rushed into the ED. You're the resident on call. The last thing on your mind is when to write progress notes.
Here's how healthcare providers can lean on AI in real time.
With Freed's instant templates, you don't need to rely on generic, pre-built formats or build every workflow from scratch. With Freed, you can bring more personalization and structure to your SOAP notes.
1. Personalized templates
Start with a Freed close to your workflow and then refine it to match your preferences. Or, upload your own note and let Freed adapt over time as you edit, helping it learn your phrasing and clinic's style.
2. Hands-free note-taking
The emergency room is fast-paced, and every second is vital. Voice-to-text recognition captures accurate, relevant notes, while you identify possible clinical complications. Keep your eyes and mind on your patient the whole time.
2. Guidelines and patient details
Pull critical patient history from past visits, as well as medical guidelines to support clinical decision-making with Freed's clinician assistant.
3. Instant, accurate codes
Generate ICD-10 and CPT codes, and E/M recommendations.
4. No more pajama time
Your work should end with your shift. By letting AI do the heavy lifting, you can quickly review your notes, then add them to your EHR with an easy integration.
Use Freed for faster documentation and CDS support
SOAP notes in EMS are necessary. But they don’t have to slow you down.
AI-powered documentation means less paperwork, more patient care.
Freed makes sure your notes keep up — so you can focus on what truly matters.
Try Freed at no cost today. No credit card required.
Table of Contents
In emergency medicine, every second counts. You're juggling critical patients, making split-second decisions, and moving fast.
There isn’t time to stop and document it all.
We’ve put together these SOAP report guidelines to help you write faster, clearer ED notes. Whether you’re working through a high-speed trauma case or a complex cardiac event, the right approach to documentation keeps your team informed and your patients safe.
Let’s break it down.
What is a SOAP narrative in EMS?
You're in the EMS— time is of the essence. You probably already have a love-hate relationship with SOAP notes.
SOAP stands for:
- Subjective: The patient’s history, symptoms, and reported concerns.
- Objective: Measurable data, including:
- Vital signs
- Lab results
- Physical exam findings
- Assessment and Plan: The clinician’s analysis of the patient’s condition and next steps for treatment or management.
SOAP notes might not be your favorite task, but they’re the glue that keeps EMS teams on the same page — even in the middle of chaos.
Don't believe me?
Check out these use cases below.
SOAP method: examples in emergency medical services
In an EMS environment, SOAP notes can bring order to the chaos. Here are some key examples:
1. EMS SOAP narrative example: Motor vehicle collision (MVC) patient
Traffic accidents are common casualties faced in the ED. Here's a sample SOAP note:
Subjective
- Patient is a 30-year-old female who arrived via ambulance after a rear-end collision.
- Reports severe neck pain and a throbbing headache since the accident.
- Denies loss of consciousness but complains of mild dizziness and nausea.
- Medical history: No known chronic conditions; no current medications.
Objective
- Vital Signs: BP 132/80 mmHg, HR 98 bpm, RR 18 breaths/min, SpO₂ 98%.
- Physical Exam:
- General: Appears alert, in moderate distress due to pain.
- Neck: Tenderness along the cervical spine, limited range of motion due to pain.
- Neuro: Cranial nerves grossly intact; no focal deficits. Normal pupil reaction.
- Skin: No significant lacerations, minor abrasions on forearm.
- Imaging: Cervical spine X-ray pending.
- Labs: Basic metabolic panel and FBC ordered; no critical abnormalities noted so far.
Assessment
- MVA (motor vehicle accident)
- Cervical strain (whiplash); no immediate evidence of fracture or intracranial injury based on initial exam.
Plan
- Continue cervical spine precautions until imaging definitively rules out fractures.
- Administer NSAIDs (e.g., ibuprofen) or acetaminophen for pain relief, considering muscle relaxants if needed.
- Observe for signs of neurological changes or increased intracranial pressure (ICP).
- If imaging is clear and patient remains stable, consider discharge with neck support and outpatient follow-up instructions.
- Counsel patient on red-flag symptoms (worsening headache, vomiting, confusion) that warrant immediate return.
2. EMS SOAP narrative example: Chest pain/possible cardiac event
Another common complaint found in the ED is the possible chest pain scenario. Here's a sample:
Subjective
- 58-year-old male presents with central, pressure-like chest pain radiating to the left arm and jaw for approximately 45 minutes.
- Reports feeling anxious, diaphoretic, and slightly nauseous.
- Past medical history: Hypertension, hyperlipidemia. Family history of coronary artery disease.
- Medications: Takes atorvastatin and lisinopril regularly.
Objective
- Vital Signs: BP 148/92 mmHg, HR 110 bpm (tachycardic), RR 20 breaths/min, SpO₂ 97% on room air.
- Physical Exam:
- General: Pale, diaphoretic, mildly anxious.
- Cardiac: Tachycardic, no significant murmurs.
- Lungs: Clear bilaterally.
- EKG: ST-segment depressions in leads II, III, and aVF (suggestive of possible ischemia).
- Labs: Cardiac enzymes (troponin) drawn; first set pending. Electrolytes within normal limits.
Assessment
- Non-ST-Elevation Acute Coronary Syndrome (NSTE-ACS) or unstable angina.
- Patient’s risk factors and EKG changes warrant urgent cardiac evaluation.
Plan
- Start IV access, place on continuous cardiac monitoring.
- Administer aspirin (chewable) if no contraindications.
- Initiate sublingual nitroglycerin if BP remains stable, and consider morphine for pain control if needed.
- Repeat EKG in 15-30 minutes.
- Consult cardiology for possible stress test or urgent catheterization based on troponin trends and patient stability.
3. EMS SOAP narrative example: Diabetic emergency (hypoglycemia)
Now, let's look at a common case of hypoglycemia.
Subjective
- 45-year-old female with Type 1 diabetes mellitus arrives confused and diaphoretic.
- Colleague states the patient was found disoriented at work, unable to recall last insulin dose or meal.
- Past medical history: Type 1 diabetes since age 15, no known diabetic complications reported.
Objective
- Vital Signs: BP 120/70 mmHg, HR 100 bpm, RR 16 breaths/min, SpO₂ 98% on room air.
- Fingerstick Glucose: 42 mg/dL (indicating hypoglycemia).
- Exam: Patient is responsive but oriented only to person, tremulous, sweaty.
- Labs: Stat BMP shows no other acute abnormalities, but awaiting additional results to rule out electrolyte imbalances.
Assessment
- Acute symptomatic hypoglycemia likely due to insulin dosing mismatch and/or inadequate dietary intake.
Plan
- Administer 25 g of 50% dextrose (D50W) IV push; recheck blood glucose in 15 minutes.
- Monitor patient’s mental status and vitals closely; initiate IV fluids if needed.
- Once stabilized, assess patient’s home insulin regimen and dietary habits; involve diabetes educator as needed.
- Consider admission if there are concerns about the patient’s ability to manage insulin dosing or social support.
These samples show one thing: organization is everything in an emergency situation.
SOAP report guidelines for EMS
In the EMS, there's no time for note bloat. Keep your progress notes clear, concise, and actionable.
Here’s how to make them work for you:
1. Keep it brief, but complete
- Focus on vital information — skip unnecessary background info.
- Use short, direct sentences to make the note easy to scan.
Example: Instead of "The patient states that they started experiencing severe chest pain about 45 minutes ago, which has been getting progressively worse," try "45M with 45 min of worsening chest pain."
2. Prioritize critical information
- In high-acuity cases, lead with the most urgent details (e.g., unstable vitals, airway concerns).
- If needed, supplement with a secondary patient care report when more time allows.
3. Use a template or EMS note-taking tool
- A structured SOAP note template keeps things efficient and consistent.
- Use the standardized format and time-saving structure to focus on key details without extra fluff.
Grab your free SOAP note template here.
4. Use standardized abbreviations
- EMS teams rely on quick, universal shorthand (e.g., SOB for shortness of breath, c/o for complaints of).
- Avoid uncommon abbreviations that could cause confusion. It's not time to reinvent the wheel.
“I make use of shorthand and common medical abbreviations. These cutbacks on words not only quicken the process of documentation but also ensure clarity in the notes.” — Dr. Sam Singh; Winit Clinic
5. Be objective and neutral
- Stick to facts and observable signs rather than assumptions.
- Instead of “patient seems intoxicated,” write “slurred speech, unsteady gait, strong odor of alcohol on breath.”
6. Ensure continuity of care
- Your SOAP note should set up the next clinician for success — whether in the ED or another facility.
- Include treatment provided, patient response, and next steps to avoid redundancy or miscommunication.
How Freed helps EMS providers document faster
AI scribes take medical dictation to the next level.
These hands-free note-taking tools are able to listen and process a conversation, turning your patient encounter into a finished medical note.
📌See how AI scribes work in ED
Benefits of using AI in EMS patient care
Multiple patients are rushed into the ED. You're the resident on call. The last thing on your mind is when to write progress notes.
Here's how healthcare providers can lean on AI in real time.
With Freed's instant templates, you don't need to rely on generic, pre-built formats or build every workflow from scratch. With Freed, you can bring more personalization and structure to your SOAP notes.
1. Personalized templates
Start with a Freed close to your workflow and then refine it to match your preferences. Or, upload your own note and let Freed adapt over time as you edit, helping it learn your phrasing and clinic's style.
2. Hands-free note-taking
The emergency room is fast-paced, and every second is vital. Voice-to-text recognition captures accurate, relevant notes, while you identify possible clinical complications. Keep your eyes and mind on your patient the whole time.
2. Guidelines and patient details
Pull critical patient history from past visits, as well as medical guidelines to support clinical decision-making with Freed's clinician assistant.
3. Instant, accurate codes
Generate ICD-10 and CPT codes, and E/M recommendations.
4. No more pajama time
Your work should end with your shift. By letting AI do the heavy lifting, you can quickly review your notes, then add them to your EHR with an easy integration.
Use Freed for faster documentation and CDS support
SOAP notes in EMS are necessary. But they don’t have to slow you down.
AI-powered documentation means less paperwork, more patient care.
Freed makes sure your notes keep up — so you can focus on what truly matters.
Try Freed at no cost today. No credit card required.
FAQs
Frequently asked questions from clinicians and medical practitioners.
What does SOAP mean in EMS?
What is the SOAP format for narratives?
How to write a good EMS narrative?
What is the EMT mnemonic for SOAP?

Related content
Free yourself for better things
548 Market Street, PMB 95301
San Francisco, CA 94104
Specialties
Compliance & Security
Our technology is HIPAA-compliant, uses industry best practices, and doesn’t store patient recordings.