10 Free Patient Notes Templates: Essential Formats for Modern Clinicians [2026]
For most clinicians, patient documentation has become a daily mental marathon that extends well beyond clinic hours.
Any night spent charting is one night too many.
If preparing patient notes is draining your mental battery, simply use patient note templates.
Be like Kevin:
I’ve curated nine plug-and-play patient note templates to speed up clinical documentation and reduce the brainpower spent in the process. Each template is designed to take the headaches out of paperwork.
9 must-have patient note templates for medical documentation
Using templates is a surefire way to reduce your documentation burden. You don’t have to start every patient note from scratch and write repetitive details over and over again.
I’ve curated nine essential clinical note templates for various use cases.
Learn the best practices for using these templates to streamline your medical documentation process across a patient’s journey.
Want to take your templates one step further?
You don’t need to rely only on pre-built formats or spend time creating your own from scratch. With Freed, you can upload or paste in a real patient note — anything from a past visit to an EHR export — and it will generate a Learned Template based on how you already document. Structured formats like SOAP notes tend to work especially well.
Explore Freed's instant templates. You can pick a format that’s close to your workflow, then shape it to fit your preferences. Or, upload your own. From there, every edit you make helps Freed fine-tune your template automatically, adapting to your phrasing, structure, and clinical style over time.
1. Patient intake form
Initial patient assessment notes, also known as intake notes, prepare the groundwork for a person’s medical record.
These comprehensive notes contain the baseline information about a patient’s condition. These details serve as a starting point for treatment plans and clinical decisions in the future.
As a best practice, you can create a standardized intake form for patients to fill out before their first visit. This allows you to reserve your documentation time for clinical impressions rather than basic data collection.
When it's used
A healthcare professional creates initial patient assessment notes during a patient’s first visit. You have to prepare these notes as a new provider to establish a reference for care plans and treatments in the future.
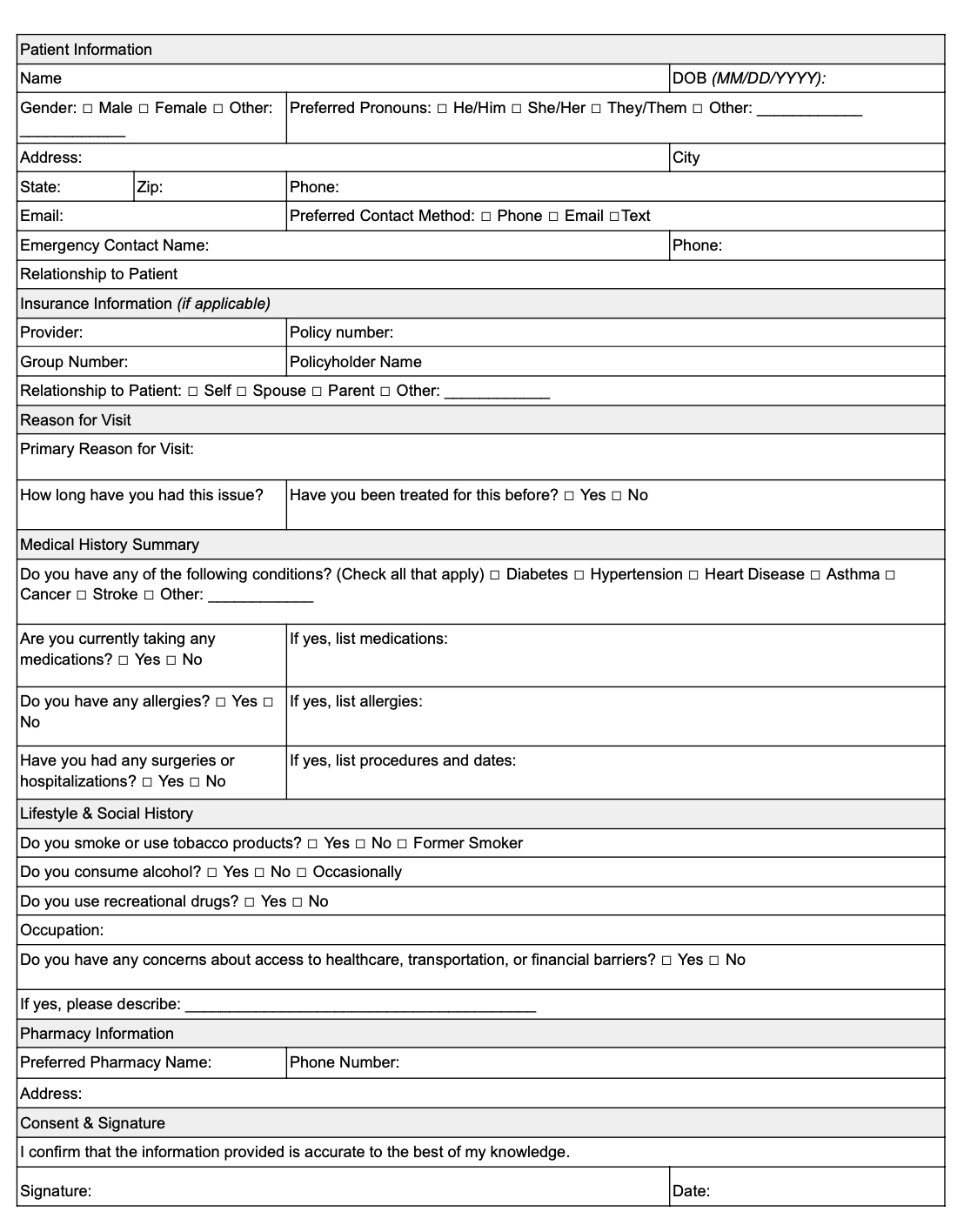
What to include in a patient intake form
Here are some key details to include in your initial assessment notes template:
- Primary concerns
- Contact information
- Patient demographics
- Current medication and allergies
- Social history, including lifestyle and habits
- Preliminary assessment and diagnostic plan
Patient intake form template
2. SOAP notes
SOAP notes, also known as progress notes, allow you to document ongoing patient care with a structured approach.
SOAP notes follow a universally recognized format—subjective, objective, assessment, and plan. That means a patient’s record will be easily understandable for every healthcare provider they interact with.
When creating SOAP notes, aim to capture subjective insights in the patient’s own words. You also need to connect subjective and objective findings to support and explain your clinical decisions.
When it’s used
These progress notes are best used for routine follow-ups and chronic disease management.
Since SOAP notes work across all specialties, any type of healthcare provider can use these notes to track patients’ conditions over time.
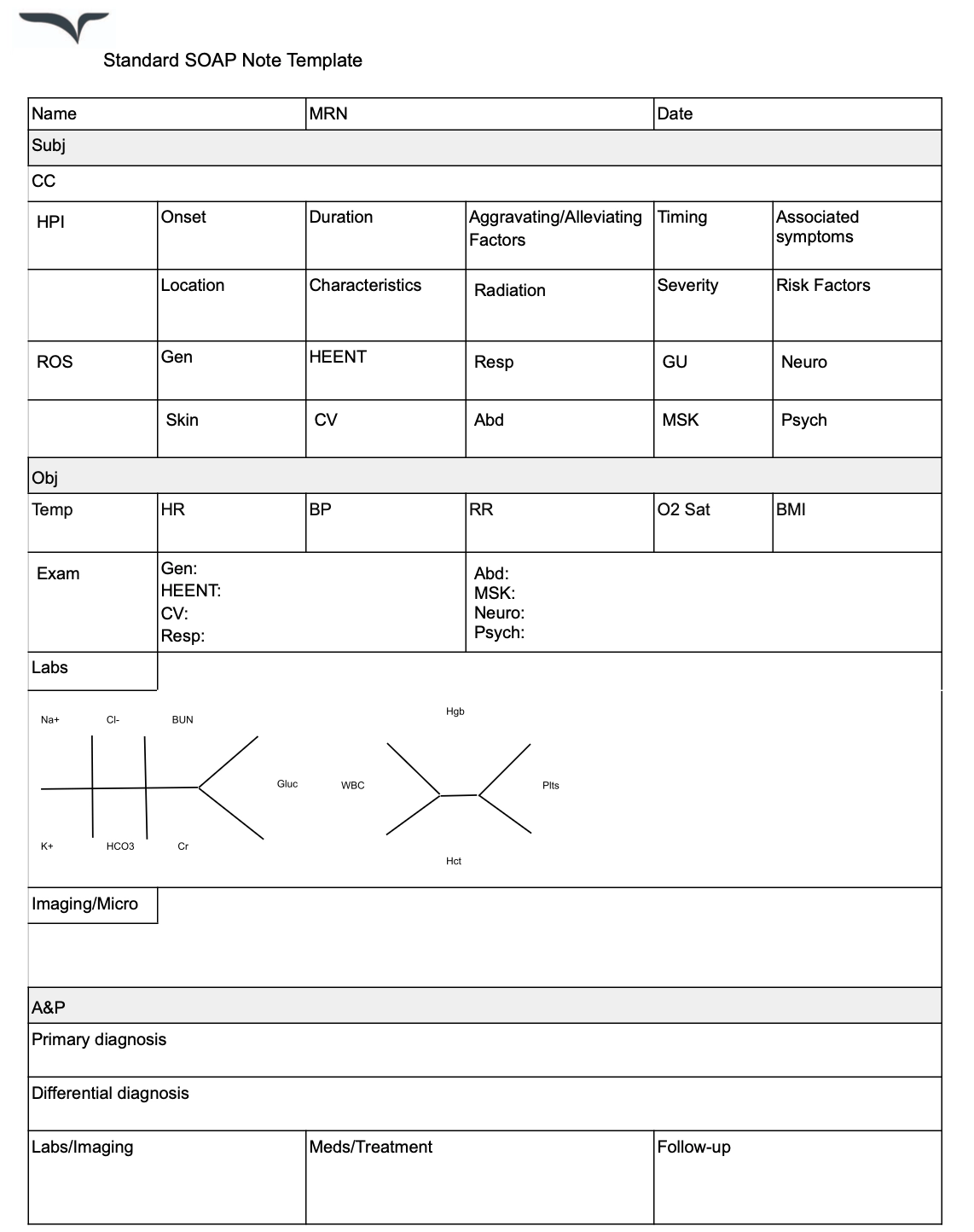
What to include in a SOAP note
Here are a few elements to include when writing SOAP notes:
- Subjective: Patient's reported symptoms, concerns, and experiences
- Objective: Measurable data ,including vital signs, physical exam findings, and test results
- Assessment: Clinical impression, diagnoses, and differential considerations
- Plan: Treatment recommendations, medications, referrals, and follow-up instructions
SOAP note template
3. Medical history form
A medical history form gathers essential details about a patient’s past and present health conditions, so you can make informed decisions about treatment and care.
This form acts is a foundation for understanding a patient’s:
- Risk factors
- Allergies
- Chronic conditions
- Previous medical interventions.
Having a standardized medical history form ensures consistency and completeness in patient records while reducing the need for repeated questioning during consultations.
When it's used
A medical history form is typically completed during a patient’s first visit or when updating their health records. It helps clinicians assess risk factors, plan treatments, and coordinate care more effectively.
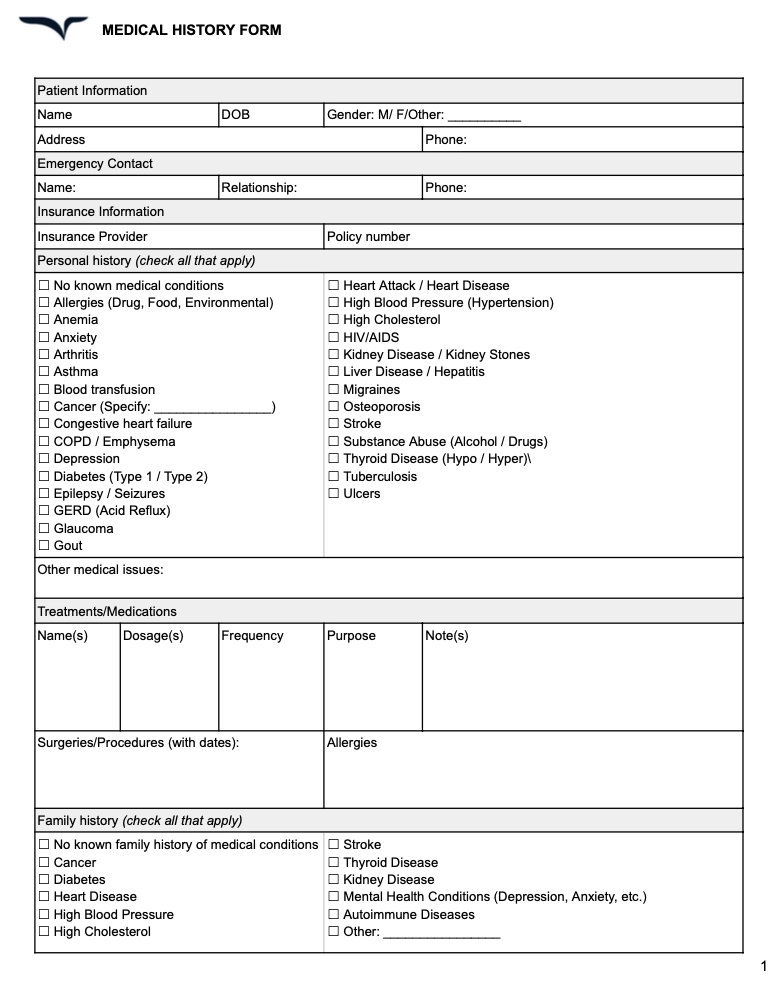
What to include in a medical history form
A comprehensive medical history form should capture:
- Personal information (name, date of birth, contact details)
- Past medical conditions (chronic illnesses, surgeries, hospitalizations)
- Family medical history (genetic predispositions, hereditary conditions)
- Current medications (prescriptions, over-the-counter drugs, supplements)
- Allergies (medications, food, environmental triggers)
- Lifestyle factors (smoking, alcohol use, exercise habits)
- Vaccination history
- Review of systems (symptoms related to different organ systems)
Free medical history form template
4. Procedure notes
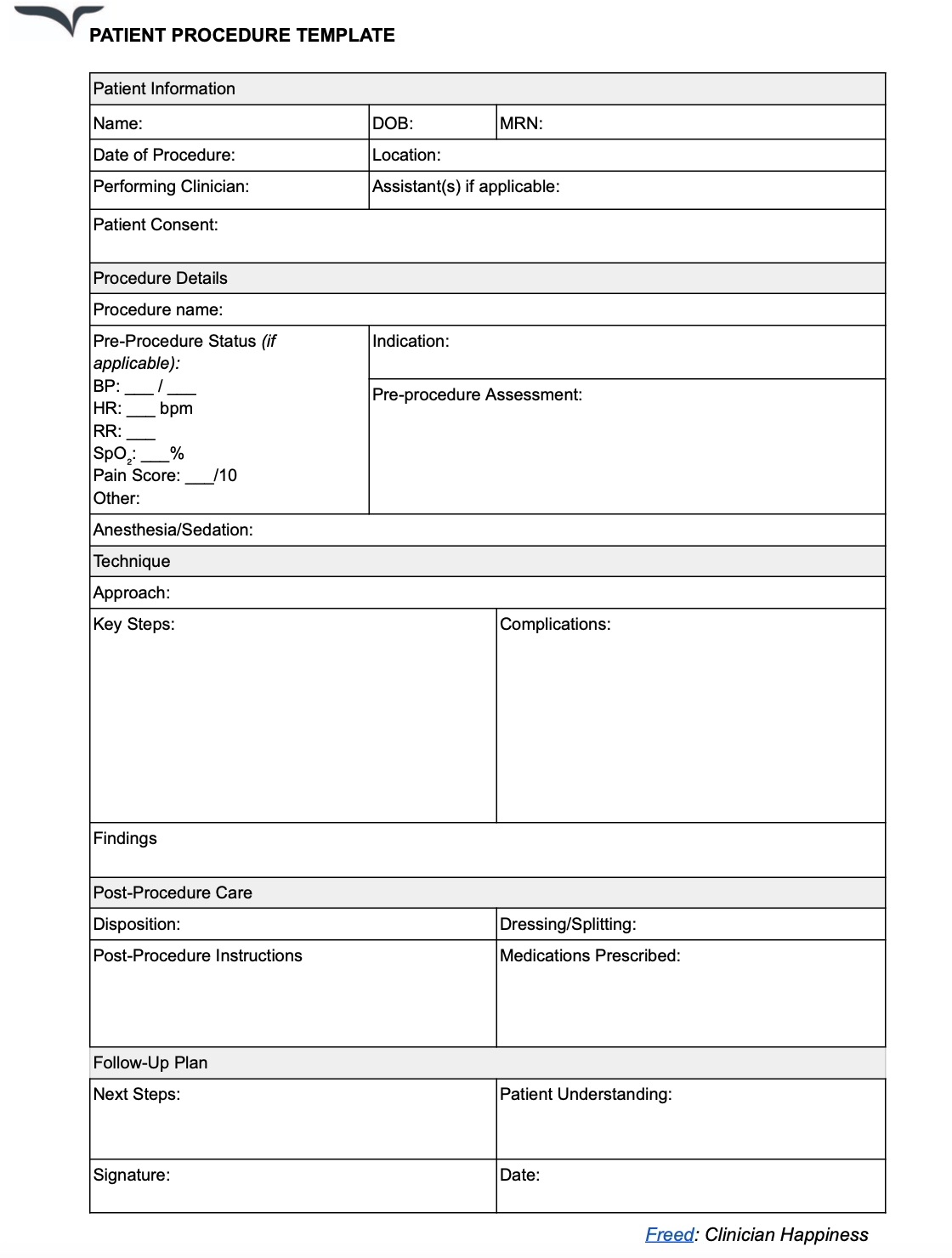
Procedure notes mention the details of the treatment performed on a patient. These notes cover every intervention during the treatment procedure. They include technical aspects, findings, and outcomes of the procedure.
Procedure notes describe the treatment technique with time-stamped steps for complex or lengthy procedures.
Clinicians also document complications during the procedure with a clear explanation of how they were addressed. You need specialty-specific templates for such patient notes.
When it's used
Procedure notes are used for all kinds of treatments — from minor in-office procedures to major surgeries. Clinicians have to complete these notes immediately for invasive procedures and diagnostic tests.
What to include in a procedure note
Here are a few essential details to add to a procedure note template:
- Informed consent document
- Pre-procedure assessment
- Procedure name and indication
- Step-by-step description of the technique
- Complications or difficulties encountered
- Post-procedure instructions and monitoring
Procedure note template
5. Discharge summary notes
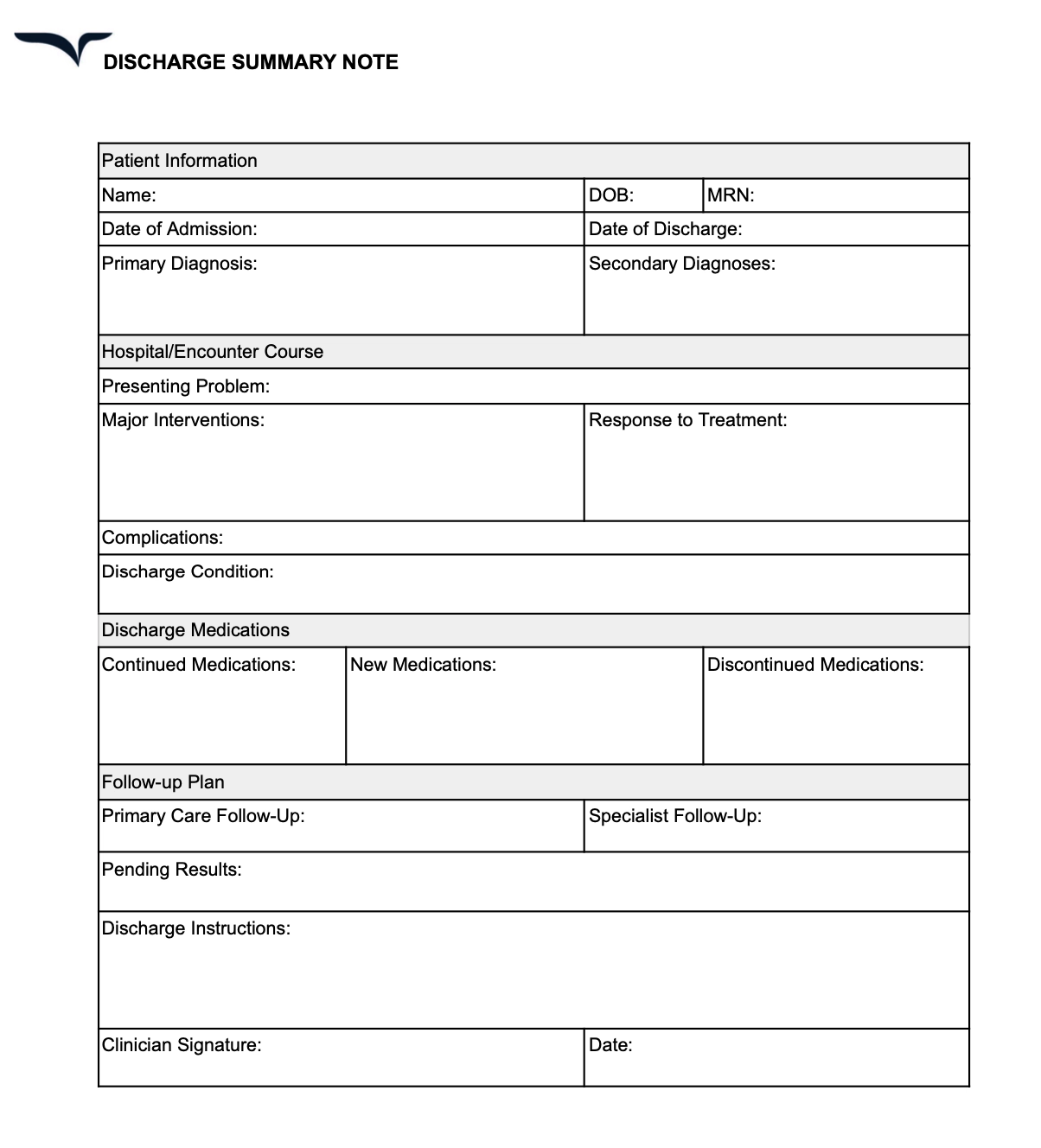
Discharge notes provide an overview of a patient’s hospital stay—treatment performed, medicines administered, and similar details. These notes also include a set of instructions for the patient’s recovery after discharge.
These notes bridge the gap between inpatient and outpatient care.
Writing clear and actionable information is important for a patient’s caretakers to continue their recovery. Clinicians have to provide simple steps and prepare a follow-up plan for future consultations.
When it’s used
Discharge summary notes are prepared when a patient has to be discharged from a hospital to a different place, like their home or a rehabilitation center.
Clinicians have to complete discharge summaries within 24 hours to ensure timely communication with follow-up providers.
What to include in a discharge summary
Here are some details to add to your discharge summary template:
- Admission date and principal diagnosis
- Overview of hospital stay
- Procedures performed and key events
- Discharge diagnoses (primary and secondary)
- Discharge medications with clear instructions
- Follow-up appointments and schedule
Discharge summary note template
6. Consultation notes
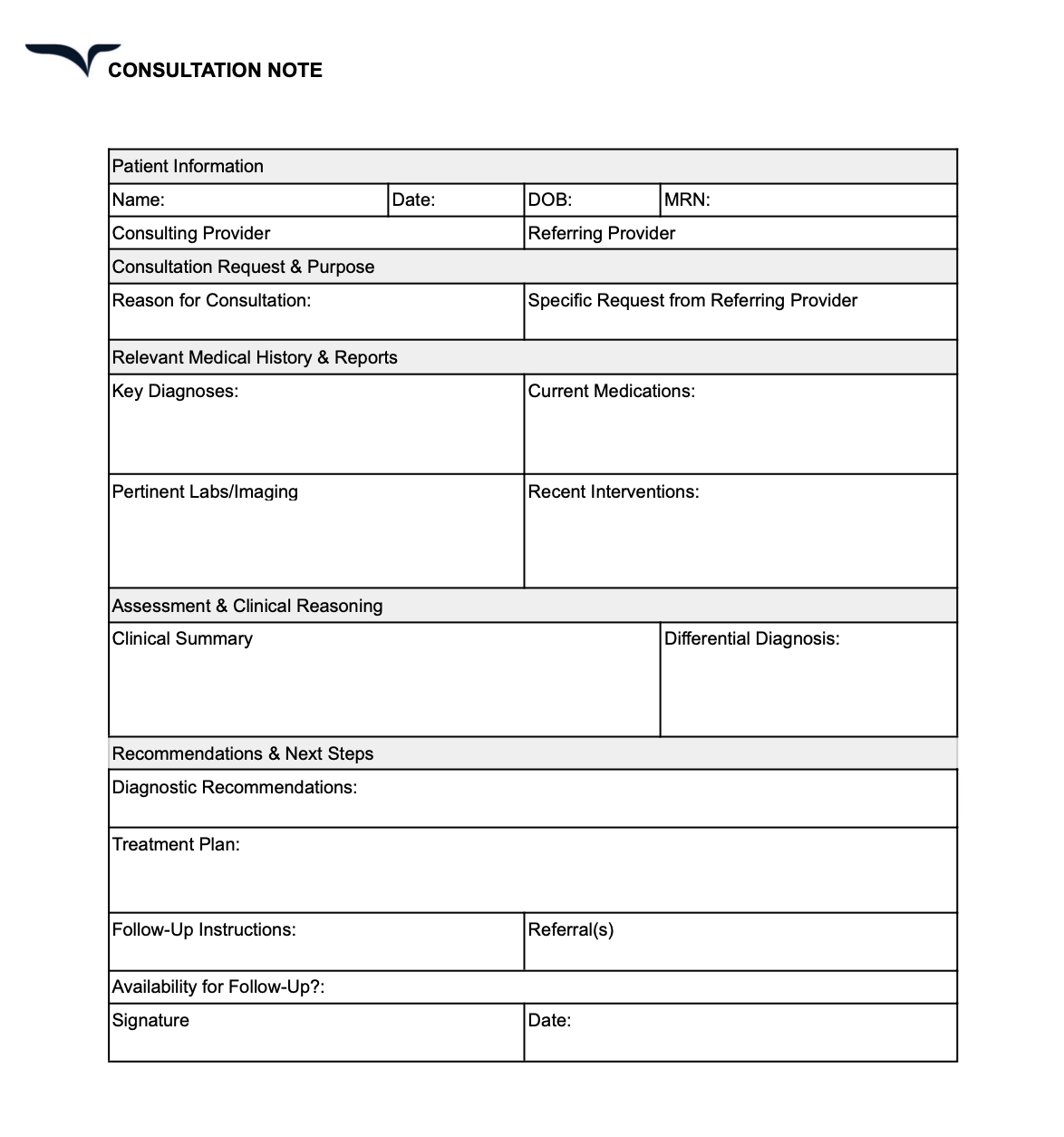
Consultation notes capture insights from a specialist’s review of a patient’s reports.
These notes facilitate communication between two or more healthcare providers about a patient. Such a note includes recommended treatments or questions from one specialist to another.
Since these notes capture different providers’ clinical reasoning, they have to use clear language to avoid any ambiguity. Clinicians should also specify whether they need a one-time consultation or continuous support from another specialist.
When it’s used
Consultation notes are used when a specialist evaluates a patient at another provider's request.
A clinician can request an evaluation of the diagnoses, procedure considerations, treatment recommendations, and other details. The consulting clinician prepares a note answering this request with detailed insights and recommendations based on their own reasoning.
What to include in a consultation note
Here’s the patient information to cover in your consultation notes template:
- Consultation purpose and request
- Patient’s medical history and relevant reports
- Assessment and clinical reasoning
- Detailed recommendations with a clear rationale
- Availability for follow-up questions
Consultation notes template
7. Telephone notes
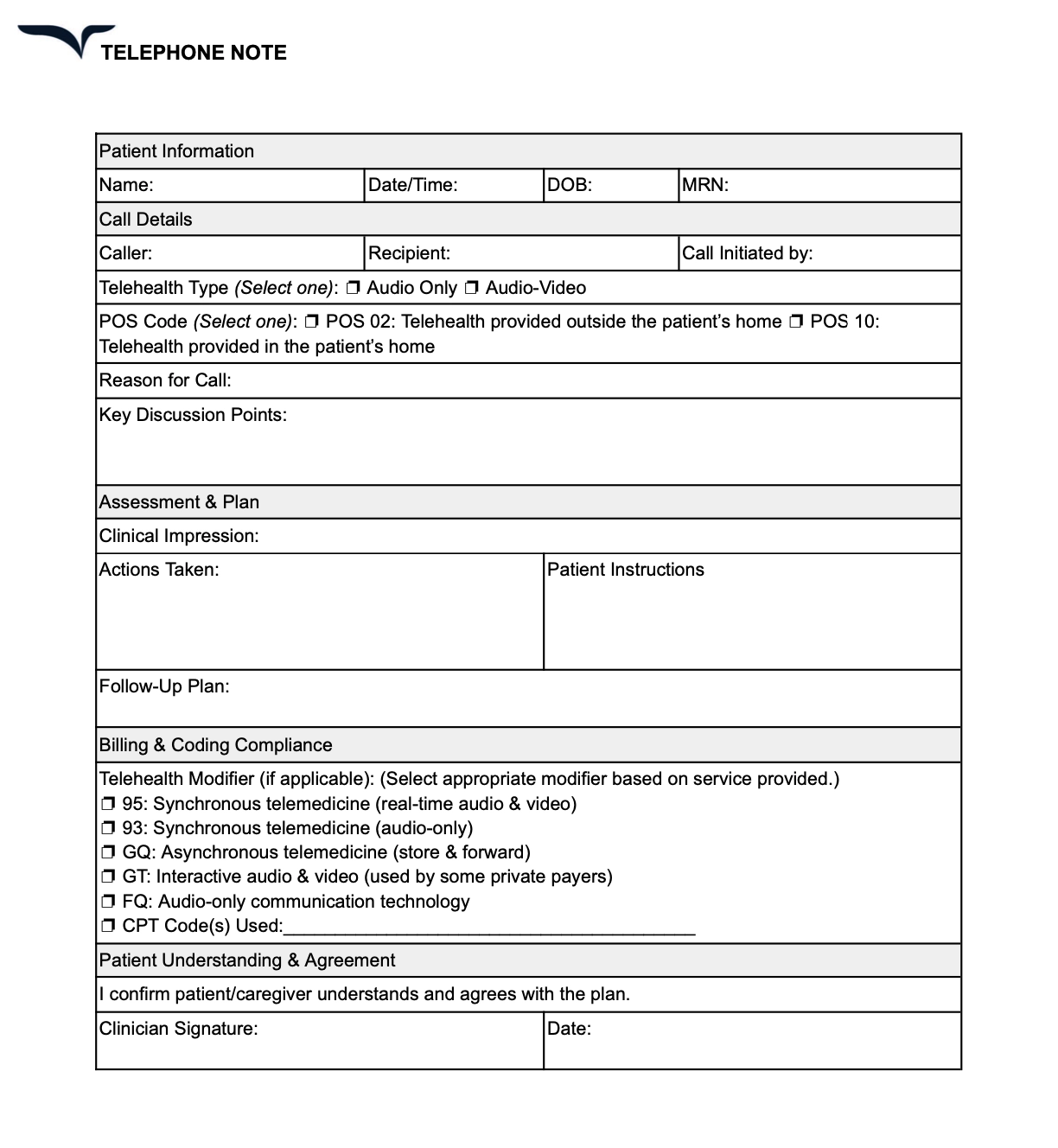
Telephone notes document remote patient visits over calls, video meetings, or messages. Used for virtual consultations, these notes document all clinical information from a patient-physician interaction.
Clinicians also need to follow telehealth billing requirements to prepare these notes.
When it’s used
Telephone notes are subjective and depend on the kind of consultation you have with patients on a call or message. That said, clinicians should prepare these notes when exchanging substantial clinical information such as:
- Prescription changes
- Follow-up test results
- Patient concerns and questions
- Pre or post-operative instructions
You should also prepare notes for information related to billing and reimbursements.
What to include in a telephone note
Here are some crucial details that go into a telephone note template:
- Consent form for tele healthcare services
- Verification of patient identity and location
- Primary complaint and focused patient history
- Assessment based on available information
Telephone notes template
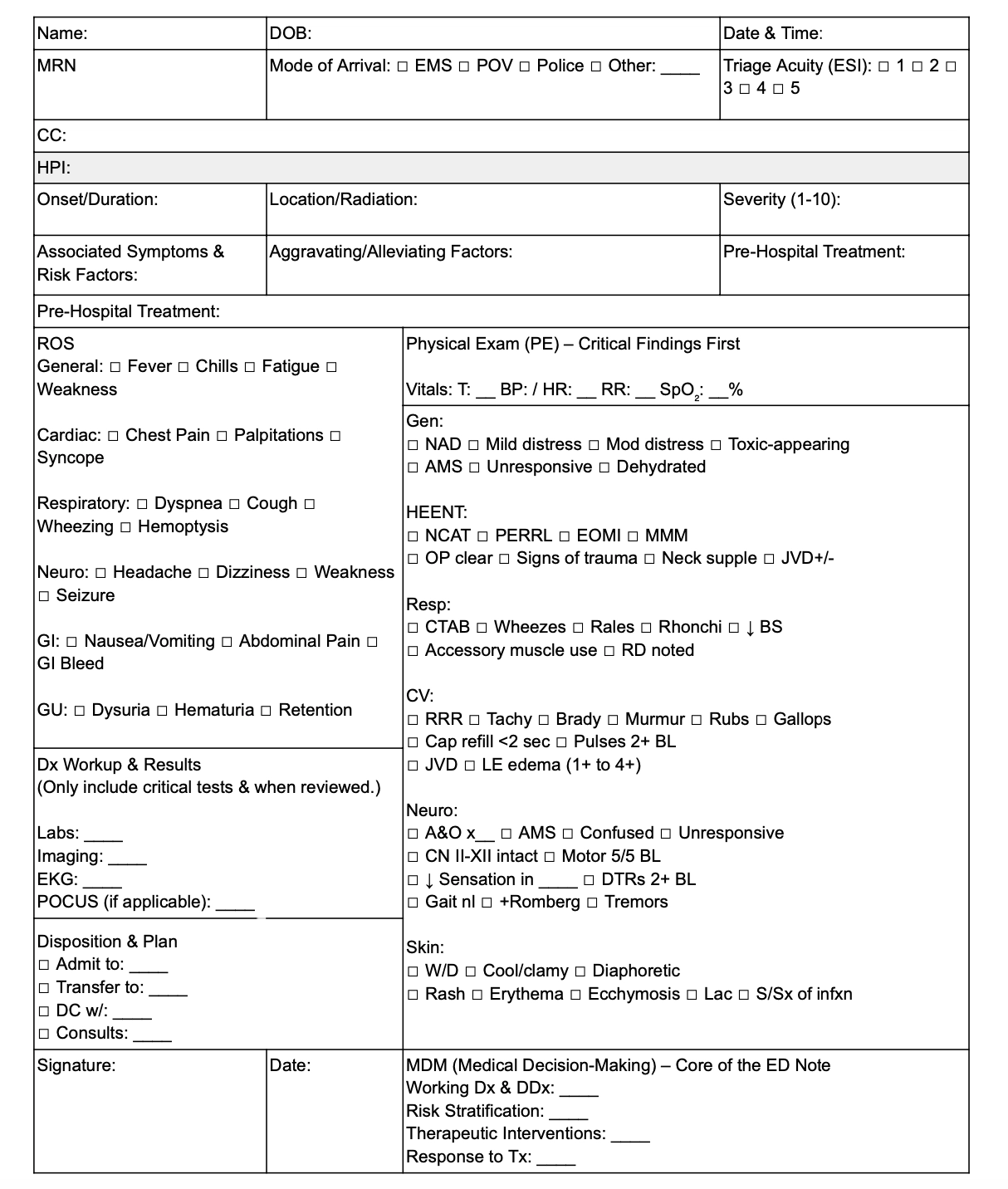
8. Emergency department notes
The emergency department notes cover time-sensitive cases and capture all the interventions performed on a patient. These notes also explain the medical decision-making process to highlight the rationale behind each intervention.
It’s best to use a chronological approach to document the progression of care in emergency scenarios.
Clinicians also prepare these notes to share their risk assessment and reasoning for each step during the procedure.
When it’s used
Emergency department notes are used to document a patient’s entire visit to the emergency room. These notes cover everything from initial presentation to discharge, admission, or transfer.
What to include in ed notes
Here are some essential details to add to emergency department notes:
- Primary concern and focused history
- Timing of key events and interventions
- Critical test results with time of review
- Medical decision-making and risk stratification
Emergency department notes template
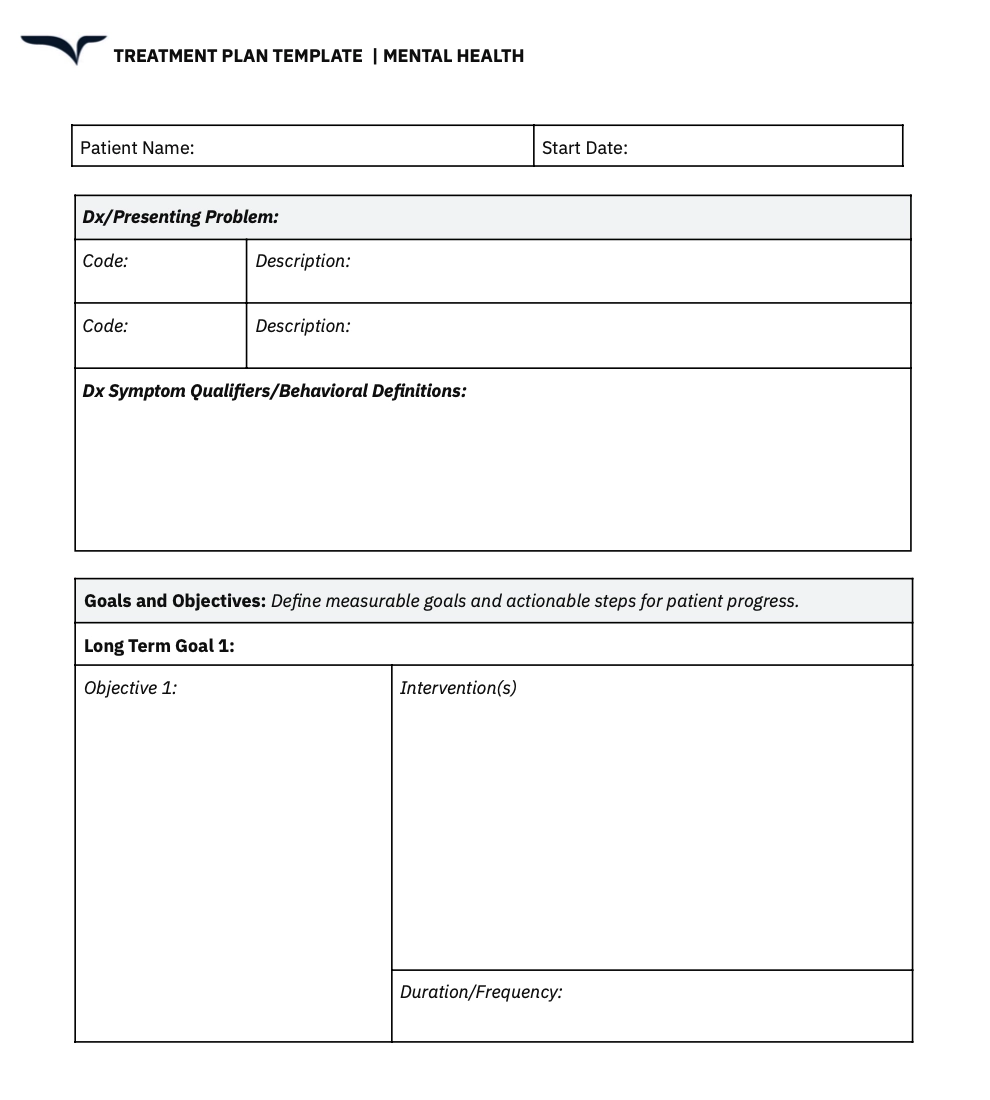
9. Mental health treatment plan
Treatment plans or mental health progress notes notes document patient care for psychological concerns.
These notes have to strictly adhere to privacy considerations and use objective language to describe patient behavior. Clinicians have to avoid judgmental terminology or subjective vocabulary.
Use these notes to document your risk assessment and substantiate it with specific statements by the patients.
When it’s used
Behavioral and mental health notes are primarily used during psychiatric evaluations and therapy sessions.
These notes are also suitable for documenting follow-up visits for chronic disease management. They help in assessing the effectiveness of the prescribed treatment and medication.
What to include in mental health notes
Here are a few elements to add to your behavioral and mental health notes template:
- Risk assessment (suicide, homicide, self-harm)
- Therapeutic interventions used and response
- Progress toward treatment goals
- Medication effects and adherence
Mental health progress treatment plan template
9. Palliative care notes
Palliative care notes, also known as end-of-life care, documents the approach of helping patients manage and live with illness that can’t be cured. It includes recommendations for symptom management to provide continuous support and enhance the quality of life.
Clinicians should use these notes to document patients' goals in their own words whenever possible. You can also add a section to focus on directives for emergency situations.
Since these notes are meant for a patient’s family and caretakers, they have to be clear and easy to understand.
When it's used
Palliative care notes document the care approach for patients with terminal illness. These notes can also be used for patients living under hospice care or going through palliative interventions alongside curative treatment.
What to include in palliative care notes
Here are the details to include in your palliative care notes template:
- Advanced care planning instructions
- Symptom management guidelines
- Comfort-focused interventions
- Changes in goals of care over time
Palliative care notes template
Use AI scribes to go beyond the manual busywork of templates
Templates are a great head start — but they’re just the beginning of smarter documentation. Freed's AI scribe doesn’t stop at giving you plug-and-play patient note formats. It turns your own templates and edits into a living system that learns how you document and evolves with your practice.
With Freed, you can:
- Upload or customize your own templates to match the exact structures you prefer (HPI ordering, unique section headers, your preferred abbreviations, and more).
- Teach Freed your style with Learn format — just edit a generated note and click Learn format, and Freed adapts future notes to match your edits.
- Tap into specialty-aware formatting and phrasing so your notes read like they were written by someone who knows your field as well as you do.
Get consistent, chart-ready notes that feel like you wrote them, without the repetitive typing or brain drain. Freed removes the busywork, learns from your edits, and streamlines documentation so you can focus on patients — and leave the office on time.
Whether you’re using these free templates as a starting point or building your own workflow-specific formats, Freed helps turn them into notes that are faster, smarter, and more personalized.
Try Freed today and see how effortless your documentation can be.
10 Free Patient Notes Templates: Essential Formats for Modern Clinicians [2026]
Table of Contents
For most clinicians, patient documentation has become a daily mental marathon that extends well beyond clinic hours.
Any night spent charting is one night too many.
If preparing patient notes is draining your mental battery, simply use patient note templates.
Be like Kevin:
I’ve curated nine plug-and-play patient note templates to speed up clinical documentation and reduce the brainpower spent in the process. Each template is designed to take the headaches out of paperwork.
9 must-have patient note templates for medical documentation
Using templates is a surefire way to reduce your documentation burden. You don’t have to start every patient note from scratch and write repetitive details over and over again.
I’ve curated nine essential clinical note templates for various use cases.
Learn the best practices for using these templates to streamline your medical documentation process across a patient’s journey.
Want to take your templates one step further?
You don’t need to rely only on pre-built formats or spend time creating your own from scratch. With Freed, you can upload or paste in a real patient note — anything from a past visit to an EHR export — and it will generate a Learned Template based on how you already document. Structured formats like SOAP notes tend to work especially well.
Explore Freed's instant templates. You can pick a format that’s close to your workflow, then shape it to fit your preferences. Or, upload your own. From there, every edit you make helps Freed fine-tune your template automatically, adapting to your phrasing, structure, and clinical style over time.
1. Patient intake form
Initial patient assessment notes, also known as intake notes, prepare the groundwork for a person’s medical record.
These comprehensive notes contain the baseline information about a patient’s condition. These details serve as a starting point for treatment plans and clinical decisions in the future.
As a best practice, you can create a standardized intake form for patients to fill out before their first visit. This allows you to reserve your documentation time for clinical impressions rather than basic data collection.
When it's used
A healthcare professional creates initial patient assessment notes during a patient’s first visit. You have to prepare these notes as a new provider to establish a reference for care plans and treatments in the future.
What to include in a patient intake form
Here are some key details to include in your initial assessment notes template:
- Primary concerns
- Contact information
- Patient demographics
- Current medication and allergies
- Social history, including lifestyle and habits
- Preliminary assessment and diagnostic plan
Patient intake form template
2. SOAP notes
SOAP notes, also known as progress notes, allow you to document ongoing patient care with a structured approach.
SOAP notes follow a universally recognized format—subjective, objective, assessment, and plan. That means a patient’s record will be easily understandable for every healthcare provider they interact with.
When creating SOAP notes, aim to capture subjective insights in the patient’s own words. You also need to connect subjective and objective findings to support and explain your clinical decisions.
When it’s used
These progress notes are best used for routine follow-ups and chronic disease management.
Since SOAP notes work across all specialties, any type of healthcare provider can use these notes to track patients’ conditions over time.
What to include in a SOAP note
Here are a few elements to include when writing SOAP notes:
- Subjective: Patient's reported symptoms, concerns, and experiences
- Objective: Measurable data ,including vital signs, physical exam findings, and test results
- Assessment: Clinical impression, diagnoses, and differential considerations
- Plan: Treatment recommendations, medications, referrals, and follow-up instructions
SOAP note template
3. Medical history form
A medical history form gathers essential details about a patient’s past and present health conditions, so you can make informed decisions about treatment and care.
This form acts is a foundation for understanding a patient’s:
- Risk factors
- Allergies
- Chronic conditions
- Previous medical interventions.
Having a standardized medical history form ensures consistency and completeness in patient records while reducing the need for repeated questioning during consultations.
When it's used
A medical history form is typically completed during a patient’s first visit or when updating their health records. It helps clinicians assess risk factors, plan treatments, and coordinate care more effectively.
What to include in a medical history form
A comprehensive medical history form should capture:
- Personal information (name, date of birth, contact details)
- Past medical conditions (chronic illnesses, surgeries, hospitalizations)
- Family medical history (genetic predispositions, hereditary conditions)
- Current medications (prescriptions, over-the-counter drugs, supplements)
- Allergies (medications, food, environmental triggers)
- Lifestyle factors (smoking, alcohol use, exercise habits)
- Vaccination history
- Review of systems (symptoms related to different organ systems)
Free medical history form template
4. Procedure notes
Procedure notes mention the details of the treatment performed on a patient. These notes cover every intervention during the treatment procedure. They include technical aspects, findings, and outcomes of the procedure.
Procedure notes describe the treatment technique with time-stamped steps for complex or lengthy procedures.
Clinicians also document complications during the procedure with a clear explanation of how they were addressed. You need specialty-specific templates for such patient notes.
When it's used
Procedure notes are used for all kinds of treatments — from minor in-office procedures to major surgeries. Clinicians have to complete these notes immediately for invasive procedures and diagnostic tests.
What to include in a procedure note
Here are a few essential details to add to a procedure note template:
- Informed consent document
- Pre-procedure assessment
- Procedure name and indication
- Step-by-step description of the technique
- Complications or difficulties encountered
- Post-procedure instructions and monitoring
Procedure note template
5. Discharge summary notes
Discharge notes provide an overview of a patient’s hospital stay—treatment performed, medicines administered, and similar details. These notes also include a set of instructions for the patient’s recovery after discharge.
These notes bridge the gap between inpatient and outpatient care.
Writing clear and actionable information is important for a patient’s caretakers to continue their recovery. Clinicians have to provide simple steps and prepare a follow-up plan for future consultations.
When it’s used
Discharge summary notes are prepared when a patient has to be discharged from a hospital to a different place, like their home or a rehabilitation center.
Clinicians have to complete discharge summaries within 24 hours to ensure timely communication with follow-up providers.
What to include in a discharge summary
Here are some details to add to your discharge summary template:
- Admission date and principal diagnosis
- Overview of hospital stay
- Procedures performed and key events
- Discharge diagnoses (primary and secondary)
- Discharge medications with clear instructions
- Follow-up appointments and schedule
Discharge summary note template
6. Consultation notes
Consultation notes capture insights from a specialist’s review of a patient’s reports.
These notes facilitate communication between two or more healthcare providers about a patient. Such a note includes recommended treatments or questions from one specialist to another.
Since these notes capture different providers’ clinical reasoning, they have to use clear language to avoid any ambiguity. Clinicians should also specify whether they need a one-time consultation or continuous support from another specialist.
When it’s used
Consultation notes are used when a specialist evaluates a patient at another provider's request.
A clinician can request an evaluation of the diagnoses, procedure considerations, treatment recommendations, and other details. The consulting clinician prepares a note answering this request with detailed insights and recommendations based on their own reasoning.
What to include in a consultation note
Here’s the patient information to cover in your consultation notes template:
- Consultation purpose and request
- Patient’s medical history and relevant reports
- Assessment and clinical reasoning
- Detailed recommendations with a clear rationale
- Availability for follow-up questions
Consultation notes template
7. Telephone notes
Telephone notes document remote patient visits over calls, video meetings, or messages. Used for virtual consultations, these notes document all clinical information from a patient-physician interaction.
Clinicians also need to follow telehealth billing requirements to prepare these notes.
When it’s used
Telephone notes are subjective and depend on the kind of consultation you have with patients on a call or message. That said, clinicians should prepare these notes when exchanging substantial clinical information such as:
- Prescription changes
- Follow-up test results
- Patient concerns and questions
- Pre or post-operative instructions
You should also prepare notes for information related to billing and reimbursements.
What to include in a telephone note
Here are some crucial details that go into a telephone note template:
- Consent form for tele healthcare services
- Verification of patient identity and location
- Primary complaint and focused patient history
- Assessment based on available information
Telephone notes template
8. Emergency department notes
The emergency department notes cover time-sensitive cases and capture all the interventions performed on a patient. These notes also explain the medical decision-making process to highlight the rationale behind each intervention.
It’s best to use a chronological approach to document the progression of care in emergency scenarios.
Clinicians also prepare these notes to share their risk assessment and reasoning for each step during the procedure.
When it’s used
Emergency department notes are used to document a patient’s entire visit to the emergency room. These notes cover everything from initial presentation to discharge, admission, or transfer.
What to include in ed notes
Here are some essential details to add to emergency department notes:
- Primary concern and focused history
- Timing of key events and interventions
- Critical test results with time of review
- Medical decision-making and risk stratification
Emergency department notes template
9. Mental health treatment plan
Treatment plans or mental health progress notes notes document patient care for psychological concerns.
These notes have to strictly adhere to privacy considerations and use objective language to describe patient behavior. Clinicians have to avoid judgmental terminology or subjective vocabulary.
Use these notes to document your risk assessment and substantiate it with specific statements by the patients.
When it’s used
Behavioral and mental health notes are primarily used during psychiatric evaluations and therapy sessions.
These notes are also suitable for documenting follow-up visits for chronic disease management. They help in assessing the effectiveness of the prescribed treatment and medication.
What to include in mental health notes
Here are a few elements to add to your behavioral and mental health notes template:
- Risk assessment (suicide, homicide, self-harm)
- Therapeutic interventions used and response
- Progress toward treatment goals
- Medication effects and adherence
Mental health progress treatment plan template
9. Palliative care notes
Palliative care notes, also known as end-of-life care, documents the approach of helping patients manage and live with illness that can’t be cured. It includes recommendations for symptom management to provide continuous support and enhance the quality of life.
Clinicians should use these notes to document patients' goals in their own words whenever possible. You can also add a section to focus on directives for emergency situations.
Since these notes are meant for a patient’s family and caretakers, they have to be clear and easy to understand.
When it's used
Palliative care notes document the care approach for patients with terminal illness. These notes can also be used for patients living under hospice care or going through palliative interventions alongside curative treatment.
What to include in palliative care notes
Here are the details to include in your palliative care notes template:
- Advanced care planning instructions
- Symptom management guidelines
- Comfort-focused interventions
- Changes in goals of care over time
Palliative care notes template
Use AI scribes to go beyond the manual busywork of templates
Templates are a great head start — but they’re just the beginning of smarter documentation. Freed's AI scribe doesn’t stop at giving you plug-and-play patient note formats. It turns your own templates and edits into a living system that learns how you document and evolves with your practice.
With Freed, you can:
- Upload or customize your own templates to match the exact structures you prefer (HPI ordering, unique section headers, your preferred abbreviations, and more).
- Teach Freed your style with Learn format — just edit a generated note and click Learn format, and Freed adapts future notes to match your edits.
- Tap into specialty-aware formatting and phrasing so your notes read like they were written by someone who knows your field as well as you do.
Get consistent, chart-ready notes that feel like you wrote them, without the repetitive typing or brain drain. Freed removes the busywork, learns from your edits, and streamlines documentation so you can focus on patients — and leave the office on time.
Whether you’re using these free templates as a starting point or building your own workflow-specific formats, Freed helps turn them into notes that are faster, smarter, and more personalized.
Try Freed today and see how effortless your documentation can be.
FAQs
Frequently asked questions from clinicians and medical practitioners.
What is the most common format for patient progress notes?
How can I make my patient notes more efficient?
Can AI scribes replace manual note-taking completely?
Q. Is my patient information safe with Freed?
Does Freed replace my medical chart template?
What should be included in a basic medical chart template?

Related content
Free yourself for better things
548 Market Street, PMB 95301
San Francisco, CA 94104
Specialties
Compliance & Security
Our technology is HIPAA-compliant, uses industry best practices, and doesn’t store patient recordings.