Patient Intake Form Templates for Faster, Simpler Intake
Good care starts long before the appointment begins.
A rushed patient intake process can lead to incomplete medical records, missing insurance details, overlooked allergies, and delayed treatment decisions. For many healthcare providers, the patient intake form is the first step in building trust.
But too often, patient intake forms become another administrative burden.
Front desk teams chase down missing contact information. Clinicians search for current medications buried in paper forms. Patients repeat their medical history multiple times. And healthcare providers lose valuable time before treatment even starts.
A well-designed patient intake form changes that.
The right medical documentation helps healthcare providers collect essential personal information, organize medical records, verify insurance coverage, document symptoms, and prepare a more informed treatment plan — before the patient ever enters the exam room.
That’s why we created a free, customizable patient intake form template designed for modern health care workflows.
Whether you run a primary care clinic, specialty practice, behavioral health office, or telehealth service, this patient intake form template helps simplify onboarding while improving documentation accuracy.
Download your free patient intake form sample template
📌 Download Now: Get a printable new client intake form PDF for easy use in your practice.
Save time with patient intake templates
You can use your real patient intake forms to make templates for future use in Freed. Just upload a note, and Freed analyzes the structure, formatting, and content. It will save the "example note" as a template that you can use for other patient encounters. Or, choose a template from Freed's comprehensive template library. Over time, Freed learns from your note edits, and will update your template accordingly.
Freed's AI scribe, paired with Freed Front desk, supports the whole patient lifecycle by enabling:
- Captured intake via automated voice
- Incorporating spoken patient details into the patient summary
- Building notes and incorporating additional context over time
Why every healthcare provider needs a structured patient intake form
A patient intake form does much more than collect paperwork.
Effective patient intake forms give healthcare providers the health information they need to deliver safer, faster, and more personalized treatment. It also improves communication between the patient, physician, nursing staff, billing teams, and administrative teams.
Without a standardized patient intake form, important details can easily fall through the cracks:
- Missing insurance policy information
- Incomplete medical history
- Incorrect phone number or address
- Undocumented allergies
- Missing emergency contact information
- Unreported symptoms
- Inaccurate medications lists
- Gaps in medical records
These issues can slow treatment, create billing challenges, and increase administrative workload across the entire health care organization.
A comprehensive patient intake form helps healthcare providers:
- Reduce repetitive data entry
- Improve medical records accuracy
- Verify insurance coverage faster
- Capture current health issues early
- Support treatment plan development
- Improve patient communication
- Streamline intake workflows
- Reduce delays during appointments
For patients, the experience feels more organized and professional. For clinicians, it means less time hunting for information and more time focused on care.
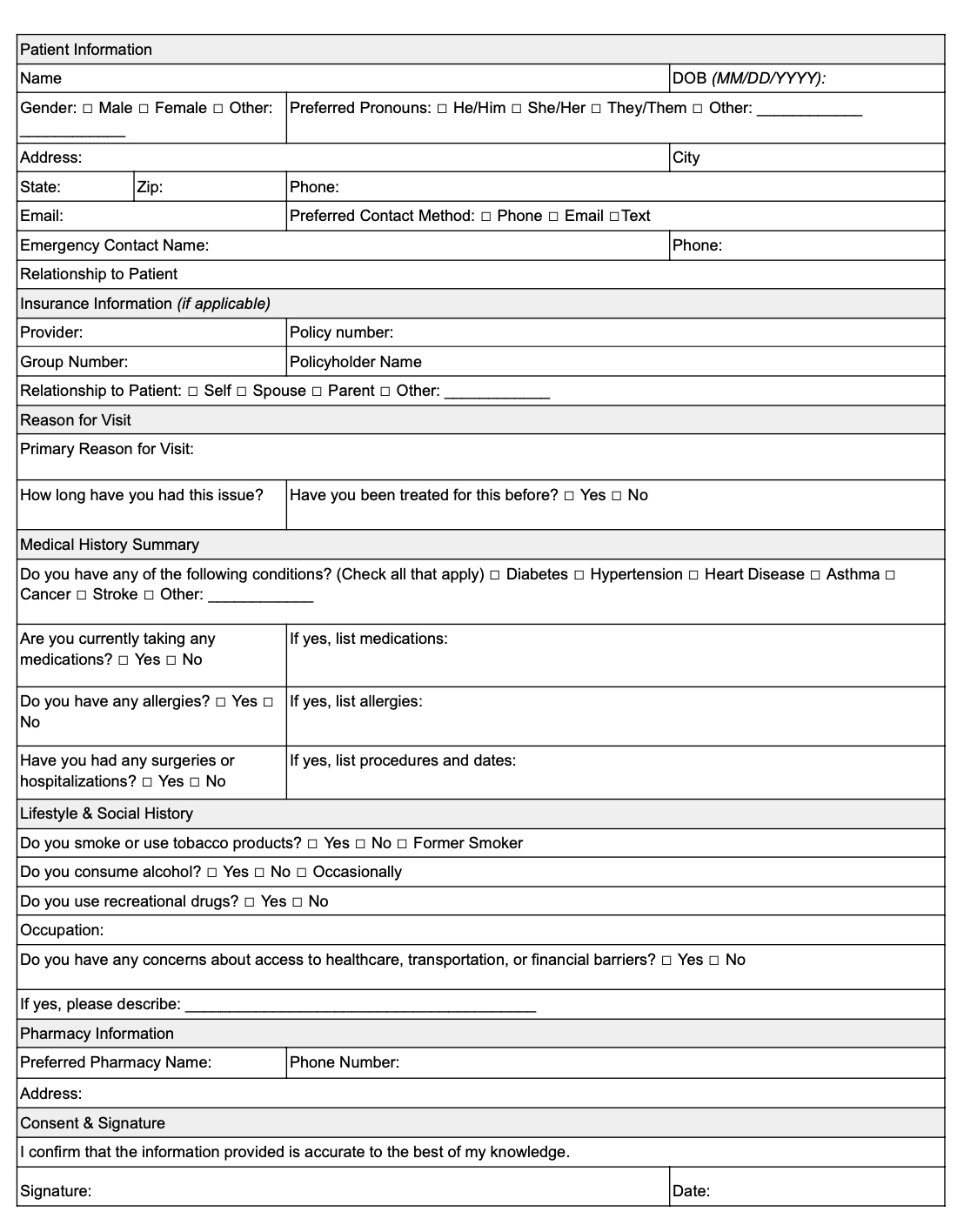
What’s inside a client intake form
A complete patient intake form should gather all relevant personal information, health information, insurance details, and medical history needed for safe and effective treatment.
Here’s what healthcare providers should include.
1. New patient information
This section typically includes:
- Full patient name
- Date of birth
- Phone number
- Email address
- Home address
- Gender
- Preferred pharmacy
- Marital status
- Employer information
Accurate contact information is essential for appointment reminders, follow-up communication, billing questions, and ongoing treatment coordination.
Healthcare providers should always confirm:
- Correct phone number
- Current address
- Updated emergency contact details
- Preferred communication method
2. Emergency contact information
Every patient intake form should include emergency contact details.
Emergency contact information may be needed during urgent treatment situations or when healthcare providers cannot reach the patient directly.
This section should include:
- Emergency contact name
- Relationship to patient
- Phone number
- Secondary phone number
- Address
- Emergency contact details for backup family members
Many healthcare providers also ask whether the emergency contact has authorization to discuss treatment or billing information.
Keeping emergency contact details current is especially important for older adults, pediatric patients, and patients with chronic health concerns.
3. Insurance information
Insurance verification is one of the most important parts of the patient intake process.
A patient intake form should capture complete insurance information to help prevent claim denials and billing delays.
Required fields often include:
- Insurance provider
- Insurance policy
- Policy number
- Group number
- Subscriber name
- Subscriber date of birth
- Secondary insurance
- Insurance phone number
Accurate insurance information helps healthcare providers confirm eligibility before treatment begins.
Missing policy number or group number information can delay reimbursement and increase administrative burden for staff.
Many patient intake forms also include a section for uploading insurance cards or attaching photos of insurance documents for digital intake workflows.
4. Medical history
Medical history is one of the most critical sections of treatment planning and risk assessment. A complete medical history gives healthcare providers insight into prior diagnoses, surgeries, chronic conditions, medications, allergies, and previous treatment decisions.
This section should include:
- Past medical history
- Current health issues
- Family Medical History
- Current medications
- Allergies
- Previous hospitalizations
- Surgical history
- Chronic conditions
- Mental health history
5. Current health issues and symptoms
A patient intake form should clearly document the patient’s current health issues and symptoms.
This section helps healthcare providers understand why the patient is seeking care and what treatment may be needed.
Questions may include:
- What symptoms are you experiencing?
- When did symptoms begin?
- Have symptoms worsened?
- Have you received prior treatment?
- Are symptoms affecting daily activities?
Healthcare providers often use this information to prioritize evaluations and begin developing a treatment plan before entering the exam room.
6. Social history
Social history provides additional context that may affect treatment outcomes and overall health care decisions.
A patient intake form may ask about:
- Tobacco use
- Alcohol use
- Drug use
- Exercise habits
- Occupation
- Living situation
- Dietary habits
Social history can help healthcare providers identify lifestyle factors connected to symptoms, chronic illness, or treatment adherence.
For example, a physician evaluating respiratory symptoms may need to know whether the patient smokes or works around environmental irritants.
7. Primary care physician information
Many patient intake forms include contact information for the patient’s primary care physician.
This supports:
- Care coordination
- Referral communication
- Medical records requests
- Shared treatment planning
Fields may include:
- Primary care physician name
- Physician phone number
- Physician address
- Referral source
For specialty clinics, obtaining primary care physician information helps maintain continuity of care across multiple healthcare providers.
8. Consent and HIPAA acknowledgment
Every patient intake form should include consent documentation.
Patients should acknowledge:
- Consent for treatment
- HIPAA privacy practices
- Financial responsibility policies
- Telehealth consent (if applicable)
- Medical records release authorization
Healthcare providers should store signed consent documentation securely within medical records systems.
This protects both the patient and the practice while supporting regulatory compliance.
What does a completed medical intake form look like?
Here’s an example of how a completed patient intake form may look.
Patient information
- Patient Name: John Doe
- Date of Birth: 01/15/1985
- Phone Number: (555) 123-4567
- Address: 123 Main Street, Springfield, IL
- Email Address: johndoe@email.com
Emergency contact details
- Emergency Contact: Jane Doe
- Relationship: Spouse
- Phone Number: (555) 987-6543
- Address: 456 Oak Avenue, Springfield, IL
Insurance information
- Insurance Provider: Blue Cross Blue Shield
- Insurance Policy: PPO Gold Plan
- Policy Number: 123456789
- Group Number: 98765
Medical history
- Past Medical History: Hypertension, Type 2 Diabetes
- Current Medications:
- Metformin
- Lisinopril
- Allergies: Penicillin
- Family Medical History:
- Father: Heart disease
- Mother: Diabetes
Current health issues
- Symptoms: Fatigue, dizziness, headaches
- Duration: Three weeks
- Previous Treatment: None
Social history
- Tobacco Use: Former smoker
- Alcohol Use: Occasional
- Exercise: Walks daily
Primary care physician
- Physician Name: Dr. Sarah Miller
- Phone Number: (555) 222-1111
Consent
- Consent for Treatment: Yes
- HIPAA Acknowledgment: Signed
Digital patient intake forms vs paper forms
Traditional paper patient intake form workflows often create unnecessary friction for both patients and healthcare providers.
Paper intake forms can lead to:
- Missing health information
- Illegible handwriting
- Incomplete insurance fields
- Delayed medical records updates
- Manual data entry errors
Digital patient intake form systems improve efficiency by allowing patients to complete forms before appointments. Benefits include:
- Faster patient onboarding
- Improved medical records accuracy
- Easier insurance verification
- Better treatment plan preparation
- Reduced front desk workload
- Faster physician review
Digital intake systems also help healthcare providers collect health information consistently across every patient encounter.
How AI clinician assistants help the patient intake process
A patient intake form is only the beginning. Modern AI scribes help healthcare providers automate documentation, organize medical history, and streamline treatment workflows in real time. Going a step further, healthcare AI agents can automate the intake process itself — sending forms, verifying insurance, and syncing responses into the EHR before the first visit.
Instead of manually reviewing paper forms, clinicians can use AI-powered tools to capture:
- Symptoms
- Current medications
- Allergies
- Medical history
- Insurance information
- Treatment plan details
Freed’s AI clinician assistant automatically structures health information into organized medical records while reducing repetitive typing and documentation burden. For example, during a new patient visit, the AI can identify:
- Current health issues
- Relevant symptoms
- Existing medications
- Prior treatment history
- Family medical history
- Physician notes
Use AI scribes for the client intake process
Forms are fine. But what if patient intake could write itself? Freed’s AI scribe captures details instantly — no typing, no hassle.
No more flipping through traditional paper forms forms or chasing down missing details. Freed’s AI scribe records everything in real time — so nothing gets lost, and you do less typing.
These AI-powered tools include:
- Auto-filled sections: Demographics, medical history, and insurance details are instantly populated.
- Seamless EHR integration: Patient data syncs directly with top electronic health records.
- Customizable fields: Adapt the form to meet your practice’s specific intake requirements.
- HIPAA-compliant security: Keeps sensitive patient information protected at all times.
- Cross-device accessibility: Use on desktops, tablets, or smartphones for in-person or virtual visits.
For example, during a new patient intake, the AI highlights allergies, current medications, and pre-existing conditions while filtering out unrelated information.
This not only speeds up the intake process but ensures clinicians have complete and accurate information — right from the start.
"I have found this to be extremely accurate and customizable. I can get a document that is arranged for an intake assessment as well as for a progress note. I can even train the scribe to write a note for counseling or psychotherapy where I don't need all of the mentions about medications, and lab work, etc because I am talking about a therapeutic issue.” — Vera T., Addictions Physician
Best practices for creating a better patient intake form
Healthcare providers should regularly review and optimize their patient intake form process.
Here are several best practices:
- Keep questions clear: Avoid overly technical language when collecting personal information or medical history.
- Minimize redundant fields: Patients should not repeat the same contact information multiple times.
- Verify insurance information: Double-check every insurance policy, policy number, and group number before appointments.
- Update medical history regularly: Medical history, medications, allergies, and symptoms can change over time.
- Make forms mobile friendly: Digital patient intake form workflows improve accessibility and completion rates.
- Protect patient privacy: Always follow HIPAA guidelines when collecting health information and storing medical records.
Download your free client intake form PDF
📌 Download Now: Click here to get the form and simplify your patient or client intake process.
Ready for faster patient intake?
Streamlined patient intake doesn’t have to mean more paperwork or lost time.
Freed can help you with patient intake through templates, our AI scribe, and other features like Freed Front Desk.
Disclaimer: This article is for informational purposes only and does not constitute legal or clinical advice. Clinicians should follow applicable laws, regulations, and institutional policies when creating or sharing intake forms.
Patient Intake Form Templates for Faster, Simpler Intake
Table of Contents
Good care starts long before the appointment begins.
A rushed patient intake process can lead to incomplete medical records, missing insurance details, overlooked allergies, and delayed treatment decisions. For many healthcare providers, the patient intake form is the first step in building trust.
But too often, patient intake forms become another administrative burden.
Front desk teams chase down missing contact information. Clinicians search for current medications buried in paper forms. Patients repeat their medical history multiple times. And healthcare providers lose valuable time before treatment even starts.
A well-designed patient intake form changes that.
The right medical documentation helps healthcare providers collect essential personal information, organize medical records, verify insurance coverage, document symptoms, and prepare a more informed treatment plan — before the patient ever enters the exam room.
That’s why we created a free, customizable patient intake form template designed for modern health care workflows.
Whether you run a primary care clinic, specialty practice, behavioral health office, or telehealth service, this patient intake form template helps simplify onboarding while improving documentation accuracy.
Download your free patient intake form sample template
📌 Download Now: Get a printable new client intake form PDF for easy use in your practice.
Save time with patient intake templates
You can use your real patient intake forms to make templates for future use in Freed. Just upload a note, and Freed analyzes the structure, formatting, and content. It will save the "example note" as a template that you can use for other patient encounters. Or, choose a template from Freed's comprehensive template library. Over time, Freed learns from your note edits, and will update your template accordingly.
Freed's AI scribe, paired with Freed Front desk, supports the whole patient lifecycle by enabling:
- Captured intake via automated voice
- Incorporating spoken patient details into the patient summary
- Building notes and incorporating additional context over time
Why every healthcare provider needs a structured patient intake form
A patient intake form does much more than collect paperwork.
Effective patient intake forms give healthcare providers the health information they need to deliver safer, faster, and more personalized treatment. It also improves communication between the patient, physician, nursing staff, billing teams, and administrative teams.
Without a standardized patient intake form, important details can easily fall through the cracks:
- Missing insurance policy information
- Incomplete medical history
- Incorrect phone number or address
- Undocumented allergies
- Missing emergency contact information
- Unreported symptoms
- Inaccurate medications lists
- Gaps in medical records
These issues can slow treatment, create billing challenges, and increase administrative workload across the entire health care organization.
A comprehensive patient intake form helps healthcare providers:
- Reduce repetitive data entry
- Improve medical records accuracy
- Verify insurance coverage faster
- Capture current health issues early
- Support treatment plan development
- Improve patient communication
- Streamline intake workflows
- Reduce delays during appointments
For patients, the experience feels more organized and professional. For clinicians, it means less time hunting for information and more time focused on care.
What’s inside a client intake form
A complete patient intake form should gather all relevant personal information, health information, insurance details, and medical history needed for safe and effective treatment.
Here’s what healthcare providers should include.
1. New patient information
This section typically includes:
- Full patient name
- Date of birth
- Phone number
- Email address
- Home address
- Gender
- Preferred pharmacy
- Marital status
- Employer information
Accurate contact information is essential for appointment reminders, follow-up communication, billing questions, and ongoing treatment coordination.
Healthcare providers should always confirm:
- Correct phone number
- Current address
- Updated emergency contact details
- Preferred communication method
2. Emergency contact information
Every patient intake form should include emergency contact details.
Emergency contact information may be needed during urgent treatment situations or when healthcare providers cannot reach the patient directly.
This section should include:
- Emergency contact name
- Relationship to patient
- Phone number
- Secondary phone number
- Address
- Emergency contact details for backup family members
Many healthcare providers also ask whether the emergency contact has authorization to discuss treatment or billing information.
Keeping emergency contact details current is especially important for older adults, pediatric patients, and patients with chronic health concerns.
3. Insurance information
Insurance verification is one of the most important parts of the patient intake process.
A patient intake form should capture complete insurance information to help prevent claim denials and billing delays.
Required fields often include:
- Insurance provider
- Insurance policy
- Policy number
- Group number
- Subscriber name
- Subscriber date of birth
- Secondary insurance
- Insurance phone number
Accurate insurance information helps healthcare providers confirm eligibility before treatment begins.
Missing policy number or group number information can delay reimbursement and increase administrative burden for staff.
Many patient intake forms also include a section for uploading insurance cards or attaching photos of insurance documents for digital intake workflows.
4. Medical history
Medical history is one of the most critical sections of treatment planning and risk assessment. A complete medical history gives healthcare providers insight into prior diagnoses, surgeries, chronic conditions, medications, allergies, and previous treatment decisions.
This section should include:
- Past medical history
- Current health issues
- Family Medical History
- Current medications
- Allergies
- Previous hospitalizations
- Surgical history
- Chronic conditions
- Mental health history
5. Current health issues and symptoms
A patient intake form should clearly document the patient’s current health issues and symptoms.
This section helps healthcare providers understand why the patient is seeking care and what treatment may be needed.
Questions may include:
- What symptoms are you experiencing?
- When did symptoms begin?
- Have symptoms worsened?
- Have you received prior treatment?
- Are symptoms affecting daily activities?
Healthcare providers often use this information to prioritize evaluations and begin developing a treatment plan before entering the exam room.
6. Social history
Social history provides additional context that may affect treatment outcomes and overall health care decisions.
A patient intake form may ask about:
- Tobacco use
- Alcohol use
- Drug use
- Exercise habits
- Occupation
- Living situation
- Dietary habits
Social history can help healthcare providers identify lifestyle factors connected to symptoms, chronic illness, or treatment adherence.
For example, a physician evaluating respiratory symptoms may need to know whether the patient smokes or works around environmental irritants.
7. Primary care physician information
Many patient intake forms include contact information for the patient’s primary care physician.
This supports:
- Care coordination
- Referral communication
- Medical records requests
- Shared treatment planning
Fields may include:
- Primary care physician name
- Physician phone number
- Physician address
- Referral source
For specialty clinics, obtaining primary care physician information helps maintain continuity of care across multiple healthcare providers.
8. Consent and HIPAA acknowledgment
Every patient intake form should include consent documentation.
Patients should acknowledge:
- Consent for treatment
- HIPAA privacy practices
- Financial responsibility policies
- Telehealth consent (if applicable)
- Medical records release authorization
Healthcare providers should store signed consent documentation securely within medical records systems.
This protects both the patient and the practice while supporting regulatory compliance.
What does a completed medical intake form look like?
Here’s an example of how a completed patient intake form may look.
Patient information
- Patient Name: John Doe
- Date of Birth: 01/15/1985
- Phone Number: (555) 123-4567
- Address: 123 Main Street, Springfield, IL
- Email Address: johndoe@email.com
Emergency contact details
- Emergency Contact: Jane Doe
- Relationship: Spouse
- Phone Number: (555) 987-6543
- Address: 456 Oak Avenue, Springfield, IL
Insurance information
- Insurance Provider: Blue Cross Blue Shield
- Insurance Policy: PPO Gold Plan
- Policy Number: 123456789
- Group Number: 98765
Medical history
- Past Medical History: Hypertension, Type 2 Diabetes
- Current Medications:
- Metformin
- Lisinopril
- Allergies: Penicillin
- Family Medical History:
- Father: Heart disease
- Mother: Diabetes
Current health issues
- Symptoms: Fatigue, dizziness, headaches
- Duration: Three weeks
- Previous Treatment: None
Social history
- Tobacco Use: Former smoker
- Alcohol Use: Occasional
- Exercise: Walks daily
Primary care physician
- Physician Name: Dr. Sarah Miller
- Phone Number: (555) 222-1111
Consent
- Consent for Treatment: Yes
- HIPAA Acknowledgment: Signed
Digital patient intake forms vs paper forms
Traditional paper patient intake form workflows often create unnecessary friction for both patients and healthcare providers.
Paper intake forms can lead to:
- Missing health information
- Illegible handwriting
- Incomplete insurance fields
- Delayed medical records updates
- Manual data entry errors
Digital patient intake form systems improve efficiency by allowing patients to complete forms before appointments. Benefits include:
- Faster patient onboarding
- Improved medical records accuracy
- Easier insurance verification
- Better treatment plan preparation
- Reduced front desk workload
- Faster physician review
Digital intake systems also help healthcare providers collect health information consistently across every patient encounter.
How AI clinician assistants help the patient intake process
A patient intake form is only the beginning. Modern AI scribes help healthcare providers automate documentation, organize medical history, and streamline treatment workflows in real time. Going a step further, healthcare AI agents can automate the intake process itself — sending forms, verifying insurance, and syncing responses into the EHR before the first visit.
Instead of manually reviewing paper forms, clinicians can use AI-powered tools to capture:
- Symptoms
- Current medications
- Allergies
- Medical history
- Insurance information
- Treatment plan details
Freed’s AI clinician assistant automatically structures health information into organized medical records while reducing repetitive typing and documentation burden. For example, during a new patient visit, the AI can identify:
- Current health issues
- Relevant symptoms
- Existing medications
- Prior treatment history
- Family medical history
- Physician notes
Use AI scribes for the client intake process
Forms are fine. But what if patient intake could write itself? Freed’s AI scribe captures details instantly — no typing, no hassle.
No more flipping through traditional paper forms forms or chasing down missing details. Freed’s AI scribe records everything in real time — so nothing gets lost, and you do less typing.
These AI-powered tools include:
- Auto-filled sections: Demographics, medical history, and insurance details are instantly populated.
- Seamless EHR integration: Patient data syncs directly with top electronic health records.
- Customizable fields: Adapt the form to meet your practice’s specific intake requirements.
- HIPAA-compliant security: Keeps sensitive patient information protected at all times.
- Cross-device accessibility: Use on desktops, tablets, or smartphones for in-person or virtual visits.
For example, during a new patient intake, the AI highlights allergies, current medications, and pre-existing conditions while filtering out unrelated information.
This not only speeds up the intake process but ensures clinicians have complete and accurate information — right from the start.
"I have found this to be extremely accurate and customizable. I can get a document that is arranged for an intake assessment as well as for a progress note. I can even train the scribe to write a note for counseling or psychotherapy where I don't need all of the mentions about medications, and lab work, etc because I am talking about a therapeutic issue.” — Vera T., Addictions Physician
Best practices for creating a better patient intake form
Healthcare providers should regularly review and optimize their patient intake form process.
Here are several best practices:
- Keep questions clear: Avoid overly technical language when collecting personal information or medical history.
- Minimize redundant fields: Patients should not repeat the same contact information multiple times.
- Verify insurance information: Double-check every insurance policy, policy number, and group number before appointments.
- Update medical history regularly: Medical history, medications, allergies, and symptoms can change over time.
- Make forms mobile friendly: Digital patient intake form workflows improve accessibility and completion rates.
- Protect patient privacy: Always follow HIPAA guidelines when collecting health information and storing medical records.
Download your free client intake form PDF
📌 Download Now: Click here to get the form and simplify your patient or client intake process.
Ready for faster patient intake?
Streamlined patient intake doesn’t have to mean more paperwork or lost time.
Freed can help you with patient intake through templates, our AI scribe, and other features like Freed Front Desk.
Disclaimer: This article is for informational purposes only and does not constitute legal or clinical advice. Clinicians should follow applicable laws, regulations, and institutional policies when creating or sharing intake forms.
FAQs
Frequently asked questions from clinicians and medical practitioners.
What is a patient intake form?
Which are examples of a patient's intake?
What is the patient intake?
What should a client intake form include?

Related content
Free yourself for better things
548 Market Street, PMB 95301
San Francisco, CA 94104
Specialties
Compliance & Security
Our technology is HIPAA-compliant, uses industry best practices, and doesn’t store patient recordings.