Free Patient Report Sheet for Nurses & Busy Clinics
Juggling multiple patients, tracking medications, and handing off care—nursing shifts move fast. And with so much to keep straight, clear documentation isn’t just helpful—it’s essential.
That’s why experienced nurses rely on a nursing report sheet — sometimes called a nurse brain sheet or patient report sheet — to stay organized throughout the day. A strong report sheet helps track medications, vitals, labs, intake and output, pending procedures, and care priorities all in one place.
Whether you work in med-surg, the ICU, pediatrics, or outpatient care, the right nursing report sheet can make patient care safer, smoother, and far less stressful.
To help, we created a free downloadable patient report sheet template designed to help nurses stay organized, improve handoff communication, and reduce documentation chaos during every shift.
Download your free nursing report sheet template
📌 Download Now: Get a printable patient report sheet to track patient details quickly and efficiently.
Want more templates?
Freed can do more than just provide you with templates. In Freed, upload or paste a sample note — like one from a past visit or your EHR — and Freed will qualify it as a learned template for you. Or, browse the Freed template library to see if there's a template you'd like to use or modify. Freed can automatically detect your edits, auto-learn, and update to match your preferred format.
Why use our nursing report sheet?
A nursing report sheet is more than a piece of paper.
It’s a cognitive support tool that helps nurses quickly prioritize patient care, track changing conditions, and communicate clearly during handoff. These "brain sheets" function like an external memory system during busy shifts.
Well-designed brain sheets help nurses:
- Stay organized during high-volume shifts
- Track medications, labs, and procedures
- Reduce missed tasks and communication errors
- Improve shift handoff accuracy
- Quickly reference patient information
- Prioritize patient care needs in real time
According to the Agency for Healthcare Research and Quality, communication breakdowns during handoff are among the leading contributors to preventable medical errors. Structured reporting tools help standardize communication and improve continuity of care.
For bedside nurses, that structure matters.
What makes a good nursing report sheet?
The best nursing report sheet templates are:
- Easy to scan quickly
- Flexible across specialties
- Organized around clinical priorities
- Designed for fast documentation
- Helpful during handoff conversations
- Built to support safe patient care
Some nurses prefer highly detailed brain sheets. Others use minimalist report sheet layouts focused only on essential patient information.
The ideal sheet depends on:
- Unit type
- Patient acuity
- Number of assigned patients
- Documentation preferences
- Handoff workflow
For example:
- ICU nurses often need space for drips, vent settings, and neuro assessments.
- Med-surg nurses may prioritize mobility, discharge planning, and medication timing.
- ER nurses typically focus on rapid assessments, diagnostics, and turnover.
What’s inside the patient report sheet?
A well-structured nursing report sheet captures critical patient information at a glance, making it easy to reference throughout your shift. Here’s what’s included:
1. Patient identification and room information
This section captures:
- Patient name and age
- Room number
- Code status
- Isolation precautions
- Date and shift assignment
Having quick access to patient information reduces confusion during fast-paced handoff situations.
2. Diagnosis and medical history
The report sheet includes dedicated space for:
- Primary diagnosis
- Relevant chronic conditions
- Surgical history
- Allergies
- Fall risk indicators
This helps nurses quickly understand the clinical picture without searching through the EHR repeatedly.
Example:
Patient: John Doe, 65M
Diagnosis: Pneumonia, COPD
History: Hypertension, Type 2 Diabetes
3. Medications and treatments
Medication management is one of the most important parts of any nursing brain sheet.
This section helps track:
- Scheduled medications
- PRN medications
- IV fluids
- Drips and infusions
- Respiratory treatments
- Pain management interventions
Example:
- Levofloxacin IV
- Albuterol nebulizer q4h
- Lisinopril 10mg daily
Keeping medication details visible on your report sheet can reduce delays and improve patient care coordination.
4. Vital signs and clinical assessments
Good brain sheets make it easy to document changing conditions quickly.
The template includes space for:
- BP
- HR
- RR
- Temperature
- O2 saturation
- Pain scores
- Neuro status
- Respiratory assessments
- Cardiac findings
Example:
- BP 130/80
- HR 78
- RR 18
- Temp 99.1°F
- O2 Sat 95% on 2L NC
This section is especially useful during handoff because incoming nurses can immediately identify trends or concerns.
5. Intake and output tracking
Fluid balance can change rapidly during a shift.
The patient report sheet includes space for:
- Oral intake
- IV intake
- Urine output
- Drain output
- Stool occurrences
- Catheter monitoring
Example:
- IV Fluids: 500mL
- Urine Output: 400mL
- Chest tube drainage: Minimal
Tracking intake and output carefully supports safer patient care decisions, especially in critical care and post-operative settings.
6. Labs, imaging, and procedures
One of the easiest ways to lose track of tasks during nursing shifts is forgetting pending tests or follow-ups.
Our nursing report sheet helps nurses stay organized by tracking:
- Pending labs
- Abnormal results
- Imaging studies
- Procedures
- Consults
- Follow-up actions
Example:
- K+ 3.1 (low) — monitor for arrhythmias
- CT chest pending
- Wound care consult ordered
7. Plan of care and handoff notes
This is one of the most important sections of any nursing brain sheet.
Effective handoff communication improves continuity and reduces preventable errors.
The template includes space for:
- Mobility status
- Diet orders
- Safety precautions
- Family updates
- Discharge planning
- Priority concerns for next shift
Example:
- Increased confusion overnight
- Monitor respiratory status closely
- Possible discharge tomorrow with home oxygen
Example of a completed nursing report sheet
Here’s an example of how a completed report sheet may look during a typical med-surg shift.
Patient Example
Patient: John Doe, 65M, Room 204
Diagnosis: Pneumonia, COPD
Vitals: Stable on 2L oxygen
Medications: Levofloxacin IV, Albuterol Neb
Labs: WBC improving
I&O: Adequate urine output
Mobility: Assist x1 with walker
Plan: Continue monitoring respiratory status
How nurses use brain sheets to stay organized
Many experienced nurses personalize their brain sheets over time.
Some use color coding. Others create symbols for common interventions. Many fold their sheet strategically to prioritize key patient information during rounds.
Here are a few ways nurses stay organized more effectively:
Use standard nursing abbreviations
Examples:
- SOB = Shortness of breath
- PRN = As needed
- AxOx3 = Alert and oriented x3
Shortened documentation saves time during busy shifts.
Focus on changes, not everything
Strong handoff communication focuses on what changed.
Instead of listing every lab:
- Highlight critical findings
- Note worsening symptoms
- Flag upcoming procedures
Example:
“K+ 3.1 — monitor cardiac rhythm.”
Update your report sheet throughout the shift
Waiting until handoff increases the risk of forgetting details.
Instead:
- Document medication responses immediately
- Add new orders in real time
- Track changing patient conditions as they happen
Example:
“10 AM: Morphine 2mg IV given.
10:30 AM: Pain improved from 8/10 to 3/10.”
Specialty-specific nursing brain sheets
Different units require different workflows.
ICU brain sheets
ICU nurses often track:
- Ventilator settings
- Vasopressors
- Sedation scores
- Neuro checks
- Hemodynamics
These brain sheets tend to be highly detailed because patient conditions change rapidly.
ER nursing report sheets
ER nurses typically prioritize:
- Chief complaint
- Triage status
- Labs and imaging
- Rapid turnover
- Disposition planning
Fast access to patient information is critical in emergency care settings.
Med-surg nursing report sheets
Med-surg report sheet templates often emphasize:
- Medication schedules
- Mobility
- Wound care
- Discharge readiness
- Fall precautions
These workflows require nurses to stay organized across multiple patients simultaneously.
Common nursing documentation mistakes
Even experienced clinicians can miss important details during stressful shifts.
Common issues include:
- Missing medication times
- Incomplete handoff notes
- Forgetting pending labs
- Delayed documentation
- Cluttered brain sheets
- Recording too much nonessential information
The best nursing report sheet templates simplify documentation while keeping essential patient information visible and actionable.
Paper brain sheets vs digital documentation
Many nurses still rely on paper brain sheets even when EHR systems are available.
Why?
Because paper allows:
- Faster note-taking
- Easier customization
- Quick visual scanning
- Real-time workflow tracking
However, digital tools are becoming increasingly valuable for reducing documentation burden and improving accuracy. The reality is that most clinicians use both.
Using AI scribes for nursing documentation
Today’s AI scribes can support nursing workflows by automatically organizing patient information into structured clinical summaries.
Instead of manually rewriting updates throughout the day, AI-powered documentation tools help nurses:
- Capture clinical conversations
- Organize patient information automatically
- Reduce repetitive charting
- Improve handoff efficiency
- Spend more time on patient care
How Freed’s AI scribe supports clinicians
Freed helps clinicians streamline documentation while maintaining HIPAA-compliant workflows.
Features include:
- Automated note organization
- EHR integrations
- Customizable templates
- Multi-device access
- Secure, HIPAA-compliant infrastructure
For example, if a patient develops worsening respiratory symptoms during a shift, the AI can highlight:
- Oxygen changes
- Respiratory assessments
- Medication updates
- New provider orders
- Relevant clinical trends
This helps nurses and clinicians stay organized without losing critical patient information during busy care transitions.
As with any documentation tool, clinicians should still review notes carefully for accuracy and completeness before finalizing records.
“I was very impressed not only with the accuracy of the notes and the format, but with the fact that the system knew what was irrelevant conversation versus medically relevant information and only relevant information made its way into the note. At the end of the visit, all I have to do is cut and paste into my note templates”. — Dr. Heather Kaufman
Download your free patient report sheet
Whether you call them brain sheets, nurse brain sheets, or nursing report sheets, the goal is the same:
Help nurses stay organized, communicate clearly, and deliver safer patient care.
📌 Download Now: Click below to get your nursing report sheet PDF and streamline your shift reports today
Taking the next step
Want more than a basic report sheet? AI scribes streamline patient reporting by capturing critical information in real time.
Because at the end of the day, it’s your expertise that makes the real difference. Documentation should work for you, not the other way around. Freed’s AI scribe captures notes in real time.
Table of Contents
Juggling multiple patients, tracking medications, and handing off care—nursing shifts move fast. And with so much to keep straight, clear documentation isn’t just helpful—it’s essential.
That’s why experienced nurses rely on a nursing report sheet — sometimes called a nurse brain sheet or patient report sheet — to stay organized throughout the day. A strong report sheet helps track medications, vitals, labs, intake and output, pending procedures, and care priorities all in one place.
Whether you work in med-surg, the ICU, pediatrics, or outpatient care, the right nursing report sheet can make patient care safer, smoother, and far less stressful.
To help, we created a free downloadable patient report sheet template designed to help nurses stay organized, improve handoff communication, and reduce documentation chaos during every shift.
Download your free nursing report sheet template
📌 Download Now: Get a printable patient report sheet to track patient details quickly and efficiently.
Want more templates?
Freed can do more than just provide you with templates. In Freed, upload or paste a sample note — like one from a past visit or your EHR — and Freed will qualify it as a learned template for you. Or, browse the Freed template library to see if there's a template you'd like to use or modify. Freed can automatically detect your edits, auto-learn, and update to match your preferred format.
Why use our nursing report sheet?
A nursing report sheet is more than a piece of paper.
It’s a cognitive support tool that helps nurses quickly prioritize patient care, track changing conditions, and communicate clearly during handoff. These "brain sheets" function like an external memory system during busy shifts.
Well-designed brain sheets help nurses:
- Stay organized during high-volume shifts
- Track medications, labs, and procedures
- Reduce missed tasks and communication errors
- Improve shift handoff accuracy
- Quickly reference patient information
- Prioritize patient care needs in real time
According to the Agency for Healthcare Research and Quality, communication breakdowns during handoff are among the leading contributors to preventable medical errors. Structured reporting tools help standardize communication and improve continuity of care.
For bedside nurses, that structure matters.
What makes a good nursing report sheet?
The best nursing report sheet templates are:
- Easy to scan quickly
- Flexible across specialties
- Organized around clinical priorities
- Designed for fast documentation
- Helpful during handoff conversations
- Built to support safe patient care
Some nurses prefer highly detailed brain sheets. Others use minimalist report sheet layouts focused only on essential patient information.
The ideal sheet depends on:
- Unit type
- Patient acuity
- Number of assigned patients
- Documentation preferences
- Handoff workflow
For example:
- ICU nurses often need space for drips, vent settings, and neuro assessments.
- Med-surg nurses may prioritize mobility, discharge planning, and medication timing.
- ER nurses typically focus on rapid assessments, diagnostics, and turnover.
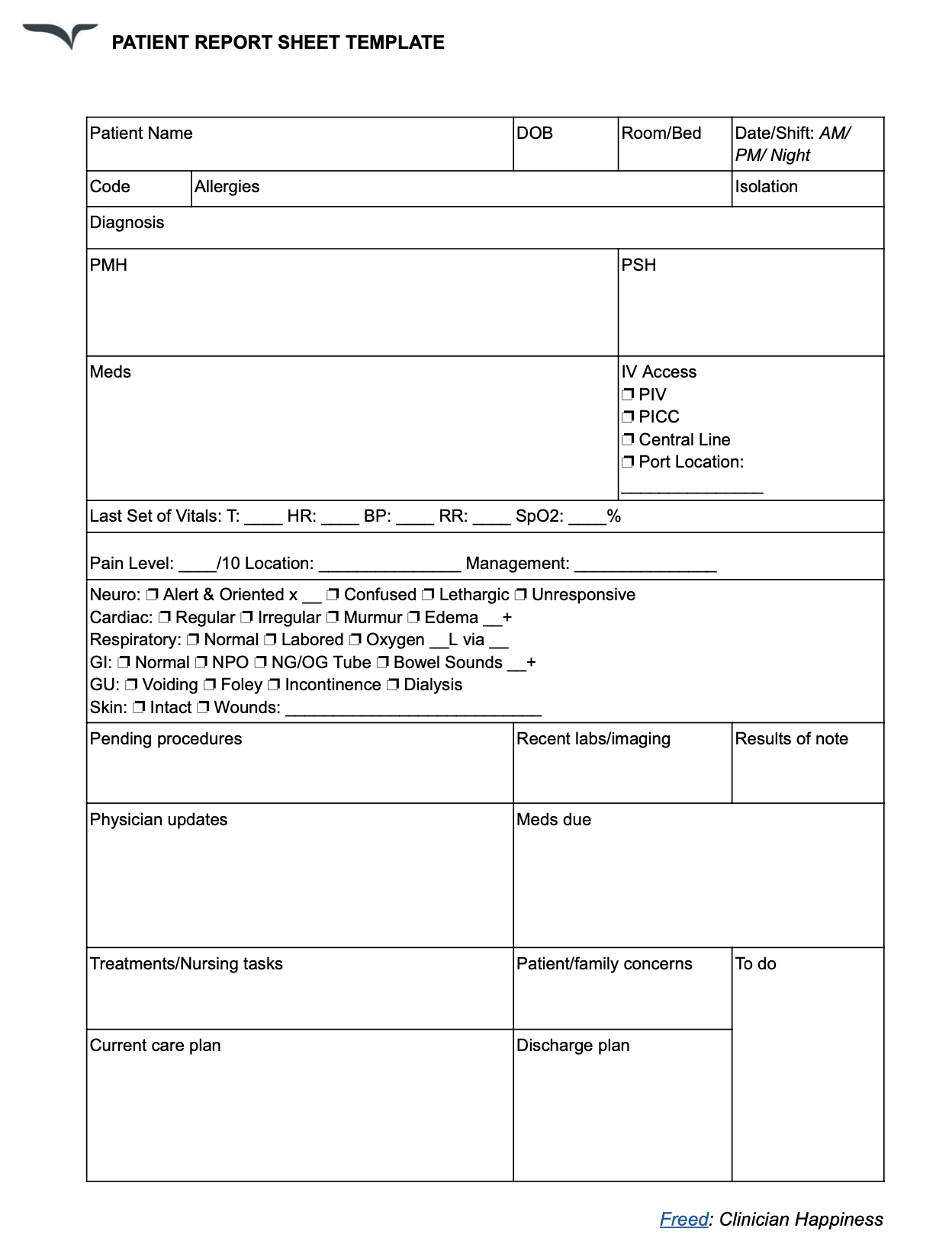
What’s inside the patient report sheet?
A well-structured nursing report sheet captures critical patient information at a glance, making it easy to reference throughout your shift. Here’s what’s included:
1. Patient identification and room information
This section captures:
- Patient name and age
- Room number
- Code status
- Isolation precautions
- Date and shift assignment
Having quick access to patient information reduces confusion during fast-paced handoff situations.
2. Diagnosis and medical history
The report sheet includes dedicated space for:
- Primary diagnosis
- Relevant chronic conditions
- Surgical history
- Allergies
- Fall risk indicators
This helps nurses quickly understand the clinical picture without searching through the EHR repeatedly.
Example:
Patient: John Doe, 65M
Diagnosis: Pneumonia, COPD
History: Hypertension, Type 2 Diabetes
3. Medications and treatments
Medication management is one of the most important parts of any nursing brain sheet.
This section helps track:
- Scheduled medications
- PRN medications
- IV fluids
- Drips and infusions
- Respiratory treatments
- Pain management interventions
Example:
- Levofloxacin IV
- Albuterol nebulizer q4h
- Lisinopril 10mg daily
Keeping medication details visible on your report sheet can reduce delays and improve patient care coordination.
4. Vital signs and clinical assessments
Good brain sheets make it easy to document changing conditions quickly.
The template includes space for:
- BP
- HR
- RR
- Temperature
- O2 saturation
- Pain scores
- Neuro status
- Respiratory assessments
- Cardiac findings
Example:
- BP 130/80
- HR 78
- RR 18
- Temp 99.1°F
- O2 Sat 95% on 2L NC
This section is especially useful during handoff because incoming nurses can immediately identify trends or concerns.
5. Intake and output tracking
Fluid balance can change rapidly during a shift.
The patient report sheet includes space for:
- Oral intake
- IV intake
- Urine output
- Drain output
- Stool occurrences
- Catheter monitoring
Example:
- IV Fluids: 500mL
- Urine Output: 400mL
- Chest tube drainage: Minimal
Tracking intake and output carefully supports safer patient care decisions, especially in critical care and post-operative settings.
6. Labs, imaging, and procedures
One of the easiest ways to lose track of tasks during nursing shifts is forgetting pending tests or follow-ups.
Our nursing report sheet helps nurses stay organized by tracking:
- Pending labs
- Abnormal results
- Imaging studies
- Procedures
- Consults
- Follow-up actions
Example:
- K+ 3.1 (low) — monitor for arrhythmias
- CT chest pending
- Wound care consult ordered
7. Plan of care and handoff notes
This is one of the most important sections of any nursing brain sheet.
Effective handoff communication improves continuity and reduces preventable errors.
The template includes space for:
- Mobility status
- Diet orders
- Safety precautions
- Family updates
- Discharge planning
- Priority concerns for next shift
Example:
- Increased confusion overnight
- Monitor respiratory status closely
- Possible discharge tomorrow with home oxygen
Example of a completed nursing report sheet
Here’s an example of how a completed report sheet may look during a typical med-surg shift.
Patient Example
Patient: John Doe, 65M, Room 204
Diagnosis: Pneumonia, COPD
Vitals: Stable on 2L oxygen
Medications: Levofloxacin IV, Albuterol Neb
Labs: WBC improving
I&O: Adequate urine output
Mobility: Assist x1 with walker
Plan: Continue monitoring respiratory status
How nurses use brain sheets to stay organized
Many experienced nurses personalize their brain sheets over time.
Some use color coding. Others create symbols for common interventions. Many fold their sheet strategically to prioritize key patient information during rounds.
Here are a few ways nurses stay organized more effectively:
Use standard nursing abbreviations
Examples:
- SOB = Shortness of breath
- PRN = As needed
- AxOx3 = Alert and oriented x3
Shortened documentation saves time during busy shifts.
Focus on changes, not everything
Strong handoff communication focuses on what changed.
Instead of listing every lab:
- Highlight critical findings
- Note worsening symptoms
- Flag upcoming procedures
Example:
“K+ 3.1 — monitor cardiac rhythm.”
Update your report sheet throughout the shift
Waiting until handoff increases the risk of forgetting details.
Instead:
- Document medication responses immediately
- Add new orders in real time
- Track changing patient conditions as they happen
Example:
“10 AM: Morphine 2mg IV given.
10:30 AM: Pain improved from 8/10 to 3/10.”
Specialty-specific nursing brain sheets
Different units require different workflows.
ICU brain sheets
ICU nurses often track:
- Ventilator settings
- Vasopressors
- Sedation scores
- Neuro checks
- Hemodynamics
These brain sheets tend to be highly detailed because patient conditions change rapidly.
ER nursing report sheets
ER nurses typically prioritize:
- Chief complaint
- Triage status
- Labs and imaging
- Rapid turnover
- Disposition planning
Fast access to patient information is critical in emergency care settings.
Med-surg nursing report sheets
Med-surg report sheet templates often emphasize:
- Medication schedules
- Mobility
- Wound care
- Discharge readiness
- Fall precautions
These workflows require nurses to stay organized across multiple patients simultaneously.
Common nursing documentation mistakes
Even experienced clinicians can miss important details during stressful shifts.
Common issues include:
- Missing medication times
- Incomplete handoff notes
- Forgetting pending labs
- Delayed documentation
- Cluttered brain sheets
- Recording too much nonessential information
The best nursing report sheet templates simplify documentation while keeping essential patient information visible and actionable.
Paper brain sheets vs digital documentation
Many nurses still rely on paper brain sheets even when EHR systems are available.
Why?
Because paper allows:
- Faster note-taking
- Easier customization
- Quick visual scanning
- Real-time workflow tracking
However, digital tools are becoming increasingly valuable for reducing documentation burden and improving accuracy. The reality is that most clinicians use both.
Using AI scribes for nursing documentation
Today’s AI scribes can support nursing workflows by automatically organizing patient information into structured clinical summaries.
Instead of manually rewriting updates throughout the day, AI-powered documentation tools help nurses:
- Capture clinical conversations
- Organize patient information automatically
- Reduce repetitive charting
- Improve handoff efficiency
- Spend more time on patient care
How Freed’s AI scribe supports clinicians
Freed helps clinicians streamline documentation while maintaining HIPAA-compliant workflows.
Features include:
- Automated note organization
- EHR integrations
- Customizable templates
- Multi-device access
- Secure, HIPAA-compliant infrastructure
For example, if a patient develops worsening respiratory symptoms during a shift, the AI can highlight:
- Oxygen changes
- Respiratory assessments
- Medication updates
- New provider orders
- Relevant clinical trends
This helps nurses and clinicians stay organized without losing critical patient information during busy care transitions.
As with any documentation tool, clinicians should still review notes carefully for accuracy and completeness before finalizing records.
“I was very impressed not only with the accuracy of the notes and the format, but with the fact that the system knew what was irrelevant conversation versus medically relevant information and only relevant information made its way into the note. At the end of the visit, all I have to do is cut and paste into my note templates”. — Dr. Heather Kaufman
Download your free patient report sheet
Whether you call them brain sheets, nurse brain sheets, or nursing report sheets, the goal is the same:
Help nurses stay organized, communicate clearly, and deliver safer patient care.
📌 Download Now: Click below to get your nursing report sheet PDF and streamline your shift reports today
Taking the next step
Want more than a basic report sheet? AI scribes streamline patient reporting by capturing critical information in real time.
Because at the end of the day, it’s your expertise that makes the real difference. Documentation should work for you, not the other way around. Freed’s AI scribe captures notes in real time.
FAQs
Frequently asked questions from clinicians and medical practitioners.
What does a nurse report sheet look like?
Where can I find free printable nursing report sheets?
What should be included on a nursing shift report sheet?
How do I make my own nursing report sheet?

Related content
Free yourself for better things
548 Market Street, PMB 95301
San Francisco, CA 94104
Specialties
Compliance & Security
Our technology is HIPAA-compliant, uses industry best practices, and doesn’t store patient recordings.