15 Medical Form Templates for a Clinical Paper Trail
Forms quietly run the world of healthcare — from the first hello to the final follow-up.
That’s why we’ve curated 15 commonly used medical form templates for every clinical need. Check out how you can use these forms to improve your patient experience and medical documentation at every step.
We'll cover five categories of form templates:
- Patient information forms
- Clinical documentation forms
- Administrative forms
- Compliance and legal forms
- Telehealth forms
Customizing your notes with Freed templates
By the way; don't want to build a template from scratch? You don't have to. In Freed, you can upload or paste in a sample note — like one from your EHR or a past visit — and Freed will instantly generate a Learned Template for you.
We recommend browsing the Freed template library first to see if something already fits, uploading your own, or simply editing one. Freed will automatically detect your edits, auto-learn, and update to match your preferred format and style.
Patient information forms
1. New patient registration form
A patient registration or intake form is often your first point of contact — capturing key info before care begins.
It collects essential details about a patient, including demographic and insurance information.
Also known as patient admission form, it starts the patient’s medical record within your system for all future interactions related to billing, appointments, and more.
When to use a new patient registration form
- Register new patients before their first appointment
- Update an existing patient’s insurance or contact info
Key elements
- Patient demographics like full legal name, address, and more
- Different contact methods and preferences
- Primary care provider information
- Current insurance policy
- HIPAA acknowledgment
Patient registration form template

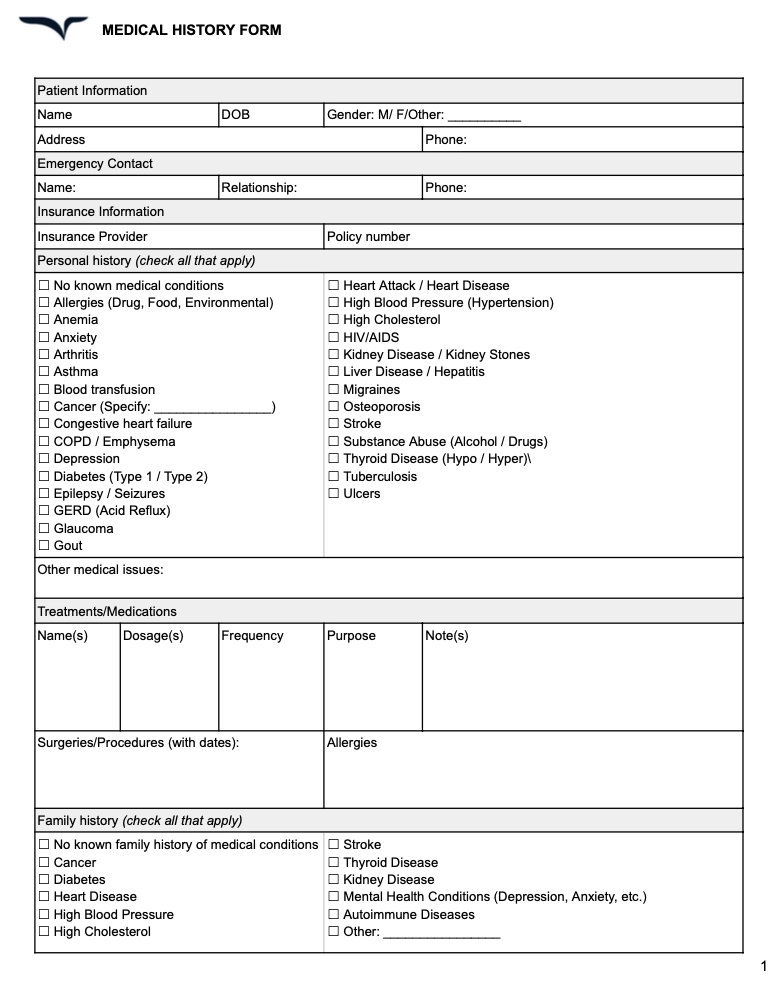
2. Medical history form
A medical history form comprehensively documents a patient’s health journey. It includes details about their past and current medical conditions, treatments, health patterns, and more.
This medical progress template form guides clinicians’ diagnostic reasoning and risk assessment. With a complete awareness of a patient’s health experiences, doctors can effectively make treatment plans and deliver more personalized care.
When to use a medical history form
- Onboarding new patients for any kind of ailment
- Preparing for surgical procedures or major treatment
- Transferring patients to a different healthcare provider
Key elements
- Personal information for identification
- List of past and present medical conditions
- History of surgical procedures with outcomes
- Data of care providers and organizations involved
- Complete medicated record with dosage and frequency
- Adverse reactions to medicines, foods, and other factors
Medical history form template
Freed template upload
One of Freed's most powerful features is its ability to adapt to the way you write notes — not the other way around. Freed offers two main template types: Learned Templates which use AI to learn from your edits and style over time, and Structured Templates, which generate notes based on a fixed outline you define.
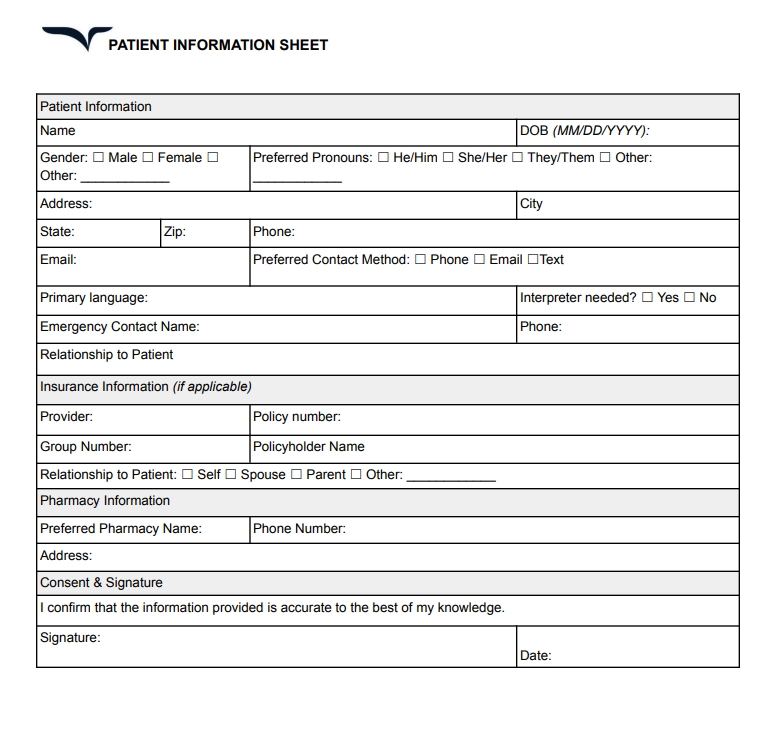
3. Patient information sheet
A patient information sheet is essential for collecting patient’s personal information for administrative purposes. It covers contact details, insurance data, emergency contacts, and other key information.
This form helps medical staff identify patients and manage their records effectively. It also ensures error-free communication and seamless operations in a healthcare setup.
When to use a patient information form
- Updating records for returning patients
- Registering new patients during their first visit
- Coordinating billing, insurance claims, and referrals
Key elements
- Full name, date of birth, contact details
- Emergency contact name and phone number
- Insurance provider, policy number, and other details
- Consent for treatment and privacy policies
Patient information form template
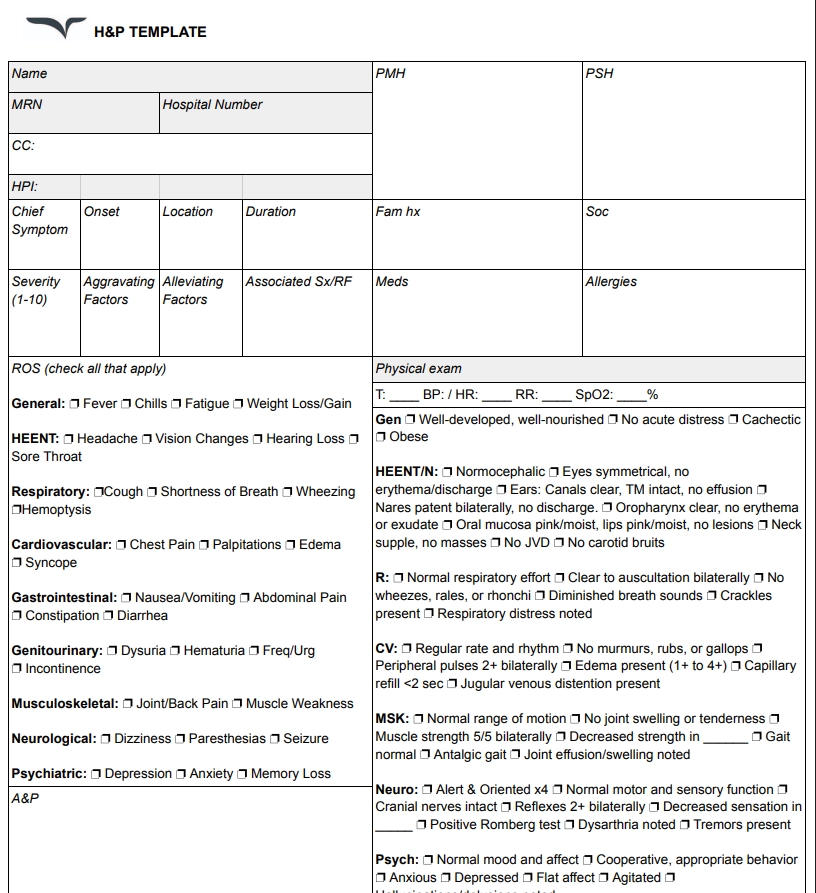
4. H&P form
An H&P (History and Physical) form includes a detailed history of a patient’s health and a summary of their physical examination. This form helps in evaluating a patient’s current health status to form diagnoses and treatment plans, especially before procedures or hospital admissions.
When to use an H&P form
- Assessing health status before surgery
- Admitting a patient to a hospital or care facility
- Documenting a new patient's complete medical evaluation
Key elements
- Chief complaint and reason for visit
- Social history including lifestyle habits
- Detailed history of present illness (HPI)
- Review of systems (ROS) and physical exam findings
H&P form template
5. Nursing report sheet
Nurses use a nursing report sheet as a quick-reference document during their shifts. It includes a summary of a patient’s current condition, care needs, and latest insights.
These forms create an efficient handoff process between nurses working different shifts. Everyone can track changes and this form ensures continuity of care.
When to use a nursing report sheet
- Tracking observations and tasks in real time
- Starting or ending a shift to brief the next nurse
- Monitoring patients in critical care or high-dependency units
Key elements
- Patient identifiers and room number
- Diagnosis and care plan
- Scheduled procedures or tests
- Vital signs and current medications
- Notes on feeding, toileting, and behavioral concerns
Nursing report form template

Clinical documentation forms
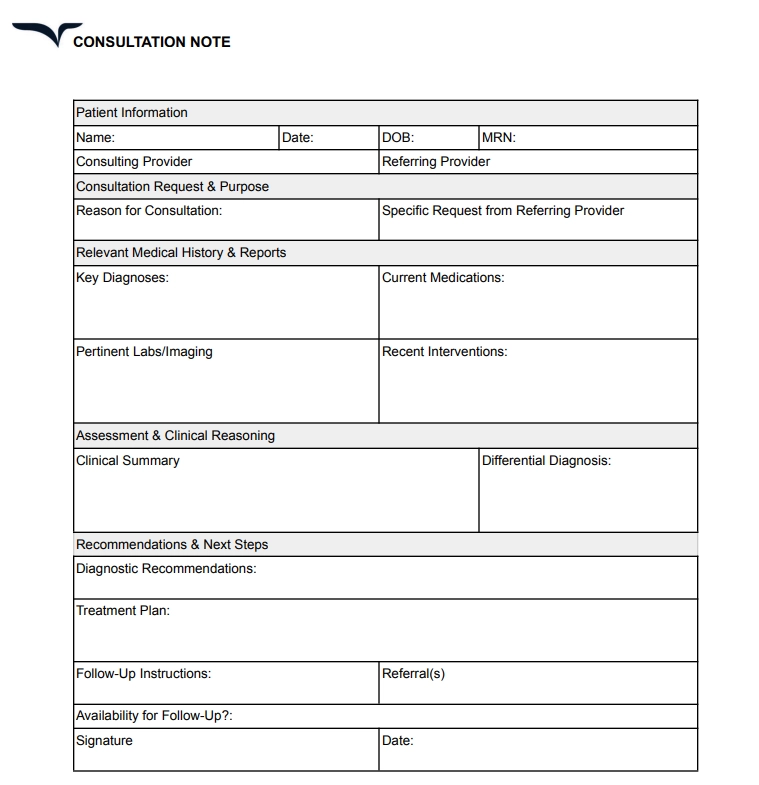
6. Consultation form
A clinical consultation form comes in handy when a clinician needs recommendations from a specialist medical professional. This form captures the insights and findings from the specialist. It systematically documents their thought process, diagnostic reasoning, and treatment planning suggestions.
Also known as a medical referral form, a consultation form enhances the coordination of care. Clinicians can consult with different specialists without losing anything in translation.
When to use a consultation form
- Referring a patient to a specialist
- Engaging in complicated clinical decision-making
- Collecting second opinions from a different provider
Key elements
- Detailed context for referring the patient
- Relevant history and medical review of the case
- Clear diagnosis and considerations with clinical reasoning
- Specific recommendations with details like timeline, re-consultation, and follow-up
Consultation form template
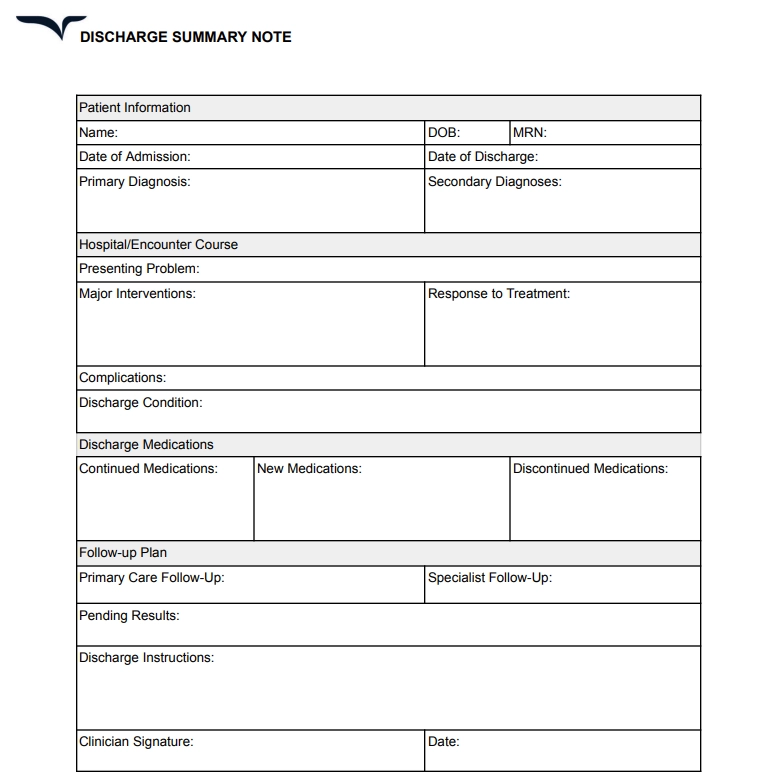
7. Patient discharge form
A discharge summary form documents a patient’s entire treatment history when admitted to a care facility. It captures critical information from their time in care and outlines instructions for post-discharge care.
A patient discharge form creates a permanent record of the diagnosis, treatment, clinician decisions, and other aspects. It supports future treatment planning.
Pair this with a medical consent form before discharging a patient.
When to use a discharge form template
- Planning a discharge from inpatient care
- Completing outpatient surgical procedures
- Transferring patients to different care facilities
Key elements
- Admission and discharge details
- Hospital stay narrative highlighting key events
- Complete list of medication with instructions
- Follow-up plan with appointments, tests, and timelines
- Patient education section for post-discharge care
Patient discharge form template
8. Physical examination form
A physical examination form is required for documenting a patient’s physical health.
This medical examination form captures the objective part of patient evaluation for SOAP notes. It provides a baseline reference of the patient’s health to support diagnostic reasoning and track progress.
When to use a physical examination form
- Preparing pre-operative assessments
- Evaluating new symptoms or conditions
- Consulting patients for the first time
Key elements
- Vital signs panel and allergy details
- Systematic exam findings with normal/abnormal status
- Standardized scoring for relevant conditions like neurological scales
Administrative forms
9. Medical records release form
A medical records release form authorizes a healthcare provider to transfer a patient’s medical records to another provider. Patients use this form to grant permission for this transfer of their protected medical information.
This form complies with HIPAA provisions by creating a paper trail of information exchange between clinicians. It works as a medical consent form.
As a result, a patient has complete control over the flow of their records.
When to use a medical records release form
- Requesting medical records from previous providers
- Patients request their information to be shared with another provider
- Releasing specially protected information (mental health, substance abuse, HIV status)
Key elements
- Details of the releasing and receiving entities
- Description of information shared with date ranges
- Patient verification with signature, date, and representative details (if applies)
- The purpose for disclosure and special authorization for sensitive information
10. Financial agreement form
A financial agreement form clarifies the financial relationship between a patient and a provider. It outlines the payment expectations and responsibilities to prevent billing conflicts and misunderstandings related to insurance.
This form aims to build a mutual understanding between both parties. It also helps patients prepare for their financial obligations by giving them a medical invoice template.
When to use a financial agreement
- Updates or changes in a patient’s insurance coverage
- Establishing payment plans for a new patient
Key elements
- Explanation of insurance billing procedures and coverage details
- Clear payment schedule with details about copays, deductibles, online bill payment timelines, and more
- Payment terms with due dates accepted payment channels and key policies
- Specific process for managing past-due accounts and potential collection actions
11. Patient satisfaction form
A patient satisfaction survey collects feedback from patients about their experience with a clinician or care facility. It captures subjective and objective data to evaluate the quality of care.
Clinicians can use this form, alongside a client history form, to identify gaps in their service and benchmark their performance against industry standards. This form can also help in improving patient experience and outcomes.
When to use a patient satisfaction survey
- Completing a major procedure
- Implementing significant practice changes
- Evaluating ongoing patient relationships at regular intervals
Key elements
- Access and convenience metrics
- Communication quality and ease metrics
- Overall care experience rating and likelihood to recommend
- Open-ended questions for specific feedback or suggestions
Compliance and legal forms
12. Incident report form
An incident report form records unexpected or adverse events in a care setting. This form captures the exact details of such incidents to serve as factual evidence in the future and potentially prevent similar mishaps.
Most organizations use incident reporting forms to clearly document errors and improve factors leading to such events.
When to use an incident report form
- Patients face complications in treatment or medication errors
- Facing unexpected clinical deterioration in patient conditions
- Equipment starts malfunctioning, or infrastructural errors happen
Key elements
- Event-specific details like date, time, location, and more
- Factual description of the incident with immediate actions taken
- Record of injuries or patient status changes and outcomes of the incident
- Immediate corrective and preventive measures for such incidents in the future
13. Durable Power of Attorney for Healthcare form
A Durable Power of Attorney for healthcare form is a legal document for designating somebody to make medical decisions if a patient becomes incapacitated and suffers from chronic illness.
This form is critical to maintain the continuity of patient care. It formally appoints a decision-making authority on behalf of the patient to prevent any dispute or confusion in a healthcare setting.
Use a Durable Power of Attorney form when
- Patients want to assign a decision-maker on their behalf
- Patients undergo a major medical procedure with significant risks
- Patients have progressive conditions that can affect their mental capacity
Key elements to include
- Designation of the decision-maker and the scope of authority granted
- Identification details of the decision-maker with different contact methods
- Conditions for activating the power of attorney and specific powers granted
Telehealth forms
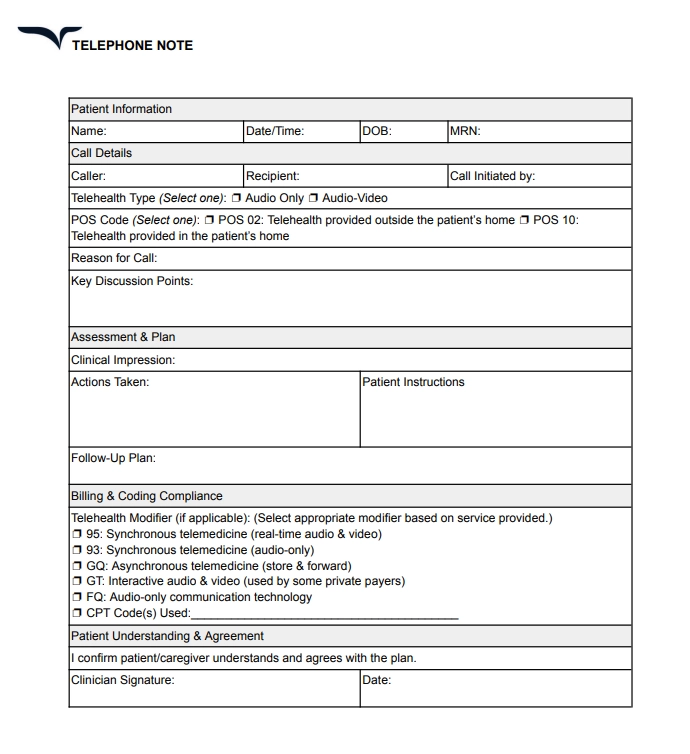
14. Telephone note
A telehealth consent form details many considerations for receiving care virtually. This online form ensures patients understand the benefits and limitations of remote care delivery.
Clinicians use this online form template to establish expectations around privacy and other protocols. It also offers clarity to help patients make informed choices when engaging with clinicians in a virtual care setting.
When to use a telephone note form
- Scheduling a virtual appointment with patients
- Changing privacy policies or tools in virtual care delivery
Key elements
- Clear privacy and security information
- Patient responsibilities and expectations
- Explanation of telehealth care’s nature, benefits, and limitations
Telehealth consent form template
15. Remote patient monitoring form
A remote patient monitoring form collects health data from wearable devices and remote equipment connected to a patient.
This online medical questionnaire helps in continuous health assessment by documenting multiple health indicators and adherence to medication. It also takes treatment consent for remote monitoring.
When to use a remote patient monitoring form
- Working on chronic illness management
- Treatment response monitoring and evaluating symptoms and medication details
- Monitoring patients during post-discharge transitional periods and timelines for patient engagement
Key elements
- Parameters monitored with normal and abnormal values
- Device specifications and data transmission process
- Intervention protocols to contact the clinicians for readings outside target ranges
Use medical form templates at every touchpoint
Medical forms create a seamless experience for both patients and providers. They capture relevant information, streamline the process of consultation, and ensure compliance with clinical guidelines.
We created these medical form templates to reduce errors and help clinicians maintain continuity of care for their patients. Designed with simplicity in mind, you can customize and use these plug-and-play templates right away in your practice.
And if you want to make paperwork even more hassle-free, let Freed do the busywork of documenting your patient interactions.
Try Freed's AI medical scribe — and spend more time on what matters, not your charts.
These templates are provided for informational purposes only and do not constitute legal or medical advice. Always consult with your healthcare organization’s compliance officer or legal team to ensure forms meet regulatory requirements and align with your specific clinical and administrative workflows.
Table of Contents
Forms quietly run the world of healthcare — from the first hello to the final follow-up.
That’s why we’ve curated 15 commonly used medical form templates for every clinical need. Check out how you can use these forms to improve your patient experience and medical documentation at every step.
We'll cover five categories of form templates:
- Patient information forms
- Clinical documentation forms
- Administrative forms
- Compliance and legal forms
- Telehealth forms
Customizing your notes with Freed templates
By the way; don't want to build a template from scratch? You don't have to. In Freed, you can upload or paste in a sample note — like one from your EHR or a past visit — and Freed will instantly generate a Learned Template for you.
We recommend browsing the Freed template library first to see if something already fits, uploading your own, or simply editing one. Freed will automatically detect your edits, auto-learn, and update to match your preferred format and style.
Patient information forms
1. New patient registration form
A patient registration or intake form is often your first point of contact — capturing key info before care begins.
It collects essential details about a patient, including demographic and insurance information.
Also known as patient admission form, it starts the patient’s medical record within your system for all future interactions related to billing, appointments, and more.
When to use a new patient registration form
- Register new patients before their first appointment
- Update an existing patient’s insurance or contact info
Key elements
- Patient demographics like full legal name, address, and more
- Different contact methods and preferences
- Primary care provider information
- Current insurance policy
- HIPAA acknowledgment
Patient registration form template
2. Medical history form
A medical history form comprehensively documents a patient’s health journey. It includes details about their past and current medical conditions, treatments, health patterns, and more.
This medical progress template form guides clinicians’ diagnostic reasoning and risk assessment. With a complete awareness of a patient’s health experiences, doctors can effectively make treatment plans and deliver more personalized care.
When to use a medical history form
- Onboarding new patients for any kind of ailment
- Preparing for surgical procedures or major treatment
- Transferring patients to a different healthcare provider
Key elements
- Personal information for identification
- List of past and present medical conditions
- History of surgical procedures with outcomes
- Data of care providers and organizations involved
- Complete medicated record with dosage and frequency
- Adverse reactions to medicines, foods, and other factors
Medical history form template
Freed template upload
One of Freed's most powerful features is its ability to adapt to the way you write notes — not the other way around. Freed offers two main template types: Learned Templates which use AI to learn from your edits and style over time, and Structured Templates, which generate notes based on a fixed outline you define.
3. Patient information sheet
A patient information sheet is essential for collecting patient’s personal information for administrative purposes. It covers contact details, insurance data, emergency contacts, and other key information.
This form helps medical staff identify patients and manage their records effectively. It also ensures error-free communication and seamless operations in a healthcare setup.
When to use a patient information form
- Updating records for returning patients
- Registering new patients during their first visit
- Coordinating billing, insurance claims, and referrals
Key elements
- Full name, date of birth, contact details
- Emergency contact name and phone number
- Insurance provider, policy number, and other details
- Consent for treatment and privacy policies
Patient information form template
4. H&P form
An H&P (History and Physical) form includes a detailed history of a patient’s health and a summary of their physical examination. This form helps in evaluating a patient’s current health status to form diagnoses and treatment plans, especially before procedures or hospital admissions.
When to use an H&P form
- Assessing health status before surgery
- Admitting a patient to a hospital or care facility
- Documenting a new patient's complete medical evaluation
Key elements
- Chief complaint and reason for visit
- Social history including lifestyle habits
- Detailed history of present illness (HPI)
- Review of systems (ROS) and physical exam findings
H&P form template
5. Nursing report sheet
Nurses use a nursing report sheet as a quick-reference document during their shifts. It includes a summary of a patient’s current condition, care needs, and latest insights.
These forms create an efficient handoff process between nurses working different shifts. Everyone can track changes and this form ensures continuity of care.
When to use a nursing report sheet
- Tracking observations and tasks in real time
- Starting or ending a shift to brief the next nurse
- Monitoring patients in critical care or high-dependency units
Key elements
- Patient identifiers and room number
- Diagnosis and care plan
- Scheduled procedures or tests
- Vital signs and current medications
- Notes on feeding, toileting, and behavioral concerns
Nursing report form template
Clinical documentation forms
6. Consultation form
A clinical consultation form comes in handy when a clinician needs recommendations from a specialist medical professional. This form captures the insights and findings from the specialist. It systematically documents their thought process, diagnostic reasoning, and treatment planning suggestions.
Also known as a medical referral form, a consultation form enhances the coordination of care. Clinicians can consult with different specialists without losing anything in translation.
When to use a consultation form
- Referring a patient to a specialist
- Engaging in complicated clinical decision-making
- Collecting second opinions from a different provider
Key elements
- Detailed context for referring the patient
- Relevant history and medical review of the case
- Clear diagnosis and considerations with clinical reasoning
- Specific recommendations with details like timeline, re-consultation, and follow-up
Consultation form template
7. Patient discharge form
A discharge summary form documents a patient’s entire treatment history when admitted to a care facility. It captures critical information from their time in care and outlines instructions for post-discharge care.
A patient discharge form creates a permanent record of the diagnosis, treatment, clinician decisions, and other aspects. It supports future treatment planning.
Pair this with a medical consent form before discharging a patient.
When to use a discharge form template
- Planning a discharge from inpatient care
- Completing outpatient surgical procedures
- Transferring patients to different care facilities
Key elements
- Admission and discharge details
- Hospital stay narrative highlighting key events
- Complete list of medication with instructions
- Follow-up plan with appointments, tests, and timelines
- Patient education section for post-discharge care
Patient discharge form template
8. Physical examination form
A physical examination form is required for documenting a patient’s physical health.
This medical examination form captures the objective part of patient evaluation for SOAP notes. It provides a baseline reference of the patient’s health to support diagnostic reasoning and track progress.
When to use a physical examination form
- Preparing pre-operative assessments
- Evaluating new symptoms or conditions
- Consulting patients for the first time
Key elements
- Vital signs panel and allergy details
- Systematic exam findings with normal/abnormal status
- Standardized scoring for relevant conditions like neurological scales
Administrative forms
9. Medical records release form
A medical records release form authorizes a healthcare provider to transfer a patient’s medical records to another provider. Patients use this form to grant permission for this transfer of their protected medical information.
This form complies with HIPAA provisions by creating a paper trail of information exchange between clinicians. It works as a medical consent form.
As a result, a patient has complete control over the flow of their records.
When to use a medical records release form
- Requesting medical records from previous providers
- Patients request their information to be shared with another provider
- Releasing specially protected information (mental health, substance abuse, HIV status)
Key elements
- Details of the releasing and receiving entities
- Description of information shared with date ranges
- Patient verification with signature, date, and representative details (if applies)
- The purpose for disclosure and special authorization for sensitive information
10. Financial agreement form
A financial agreement form clarifies the financial relationship between a patient and a provider. It outlines the payment expectations and responsibilities to prevent billing conflicts and misunderstandings related to insurance.
This form aims to build a mutual understanding between both parties. It also helps patients prepare for their financial obligations by giving them a medical invoice template.
When to use a financial agreement
- Updates or changes in a patient’s insurance coverage
- Establishing payment plans for a new patient
Key elements
- Explanation of insurance billing procedures and coverage details
- Clear payment schedule with details about copays, deductibles, online bill payment timelines, and more
- Payment terms with due dates accepted payment channels and key policies
- Specific process for managing past-due accounts and potential collection actions
11. Patient satisfaction form
A patient satisfaction survey collects feedback from patients about their experience with a clinician or care facility. It captures subjective and objective data to evaluate the quality of care.
Clinicians can use this form, alongside a client history form, to identify gaps in their service and benchmark their performance against industry standards. This form can also help in improving patient experience and outcomes.
When to use a patient satisfaction survey
- Completing a major procedure
- Implementing significant practice changes
- Evaluating ongoing patient relationships at regular intervals
Key elements
- Access and convenience metrics
- Communication quality and ease metrics
- Overall care experience rating and likelihood to recommend
- Open-ended questions for specific feedback or suggestions
Compliance and legal forms
12. Incident report form
An incident report form records unexpected or adverse events in a care setting. This form captures the exact details of such incidents to serve as factual evidence in the future and potentially prevent similar mishaps.
Most organizations use incident reporting forms to clearly document errors and improve factors leading to such events.
When to use an incident report form
- Patients face complications in treatment or medication errors
- Facing unexpected clinical deterioration in patient conditions
- Equipment starts malfunctioning, or infrastructural errors happen
Key elements
- Event-specific details like date, time, location, and more
- Factual description of the incident with immediate actions taken
- Record of injuries or patient status changes and outcomes of the incident
- Immediate corrective and preventive measures for such incidents in the future
13. Durable Power of Attorney for Healthcare form
A Durable Power of Attorney for healthcare form is a legal document for designating somebody to make medical decisions if a patient becomes incapacitated and suffers from chronic illness.
This form is critical to maintain the continuity of patient care. It formally appoints a decision-making authority on behalf of the patient to prevent any dispute or confusion in a healthcare setting.
Use a Durable Power of Attorney form when
- Patients want to assign a decision-maker on their behalf
- Patients undergo a major medical procedure with significant risks
- Patients have progressive conditions that can affect their mental capacity
Key elements to include
- Designation of the decision-maker and the scope of authority granted
- Identification details of the decision-maker with different contact methods
- Conditions for activating the power of attorney and specific powers granted
Telehealth forms
14. Telephone note
A telehealth consent form details many considerations for receiving care virtually. This online form ensures patients understand the benefits and limitations of remote care delivery.
Clinicians use this online form template to establish expectations around privacy and other protocols. It also offers clarity to help patients make informed choices when engaging with clinicians in a virtual care setting.
When to use a telephone note form
- Scheduling a virtual appointment with patients
- Changing privacy policies or tools in virtual care delivery
Key elements
- Clear privacy and security information
- Patient responsibilities and expectations
- Explanation of telehealth care’s nature, benefits, and limitations
Telehealth consent form template
15. Remote patient monitoring form
A remote patient monitoring form collects health data from wearable devices and remote equipment connected to a patient.
This online medical questionnaire helps in continuous health assessment by documenting multiple health indicators and adherence to medication. It also takes treatment consent for remote monitoring.
When to use a remote patient monitoring form
- Working on chronic illness management
- Treatment response monitoring and evaluating symptoms and medication details
- Monitoring patients during post-discharge transitional periods and timelines for patient engagement
Key elements
- Parameters monitored with normal and abnormal values
- Device specifications and data transmission process
- Intervention protocols to contact the clinicians for readings outside target ranges
Use medical form templates at every touchpoint
Medical forms create a seamless experience for both patients and providers. They capture relevant information, streamline the process of consultation, and ensure compliance with clinical guidelines.
We created these medical form templates to reduce errors and help clinicians maintain continuity of care for their patients. Designed with simplicity in mind, you can customize and use these plug-and-play templates right away in your practice.
And if you want to make paperwork even more hassle-free, let Freed do the busywork of documenting your patient interactions.
Try Freed's AI medical scribe — and spend more time on what matters, not your charts.
These templates are provided for informational purposes only and do not constitute legal or medical advice. Always consult with your healthcare organization’s compliance officer or legal team to ensure forms meet regulatory requirements and align with your specific clinical and administrative workflows.
FAQs
Frequently asked questions from clinicians and medical practitioners.
Is there a collection of minimalist note templates?
Are AI tools better than static templates for medical notes?
What’s the difference between an online template and a paper form?
How can an organization improve teamwork using online templates?
Does Freed replace my medical chart template?
How can I get started with Freed?
.avif)
Related content
Free yourself for better things
548 Market Street, PMB 95301
San Francisco, CA 94104
Specialties
Compliance & Security
Our technology is HIPAA-compliant, uses industry best practices, and doesn’t store patient recordings.