Clinical Summary Template, Samples, & Best Practices
77.42% of health professionals say they're finishing work later than desired. Why? Excessive documentation tasks.
Too much clinical documentation drives work after-hours, burnout, and less time with patients. NIH research on EHR burden shows that documentation tasks often spill beyond the workday. And yet, the clinical summary remains one of the most important parts of patient care.
A well-written clinical summary gives every health care provider a quick, accurate view of the patient’s medical history, presenting problem, symptoms, diagnosis, treatment history, current medications, clinical findings, patient progress, and follow-up care recommendations. It supports continuity of care, improves communication, and helps ensure every treatment plan is based on complete health information.
The challenge is that writing a comprehensive clinical summary takes time.
That’s why we created this guide.
Inside, you’ll find:
- A downloadable clinical summary template
- Examples of effective clinical documentation
- Best practices for organizing patient information
- Specialty-specific considerations
- Common mistakes to avoid
- Guidance on HIPAA-compliant AI scribes
- A real-world clinical summary example
- Tips for improving patient progress tracking and follow-up care
Whether you work in primary care, mental health, urgent care, or specialty medicine, this guide will help you create more efficient, accurate, and useful clinical summaries.
What is a clinical summary?
A clinical summary is a concise but comprehensive overview of a patient's medical history, their encounter, diagnosis, treatment, and ongoing care plan.
It captures the most important patient information from a visit and organizes it into a format that allows another health care provider to quickly understand the patient’s medical history, presenting problem, symptoms, assessment, treatment history, current medications, clinical findings, recommendations, and follow-up care plan.
A clinical summary may be used during:
- Routine office visits
- Specialist consultations
- Mental health evaluations
- Discharge summary documentation
- Transitions of care
- Emergency department visits
- Hospital admissions
- Follow-up appointments
- Referral coordination
In many organizations, the clinical summary also becomes part of the permanent medical records. Because of this, accurate clinical documentation is essential.
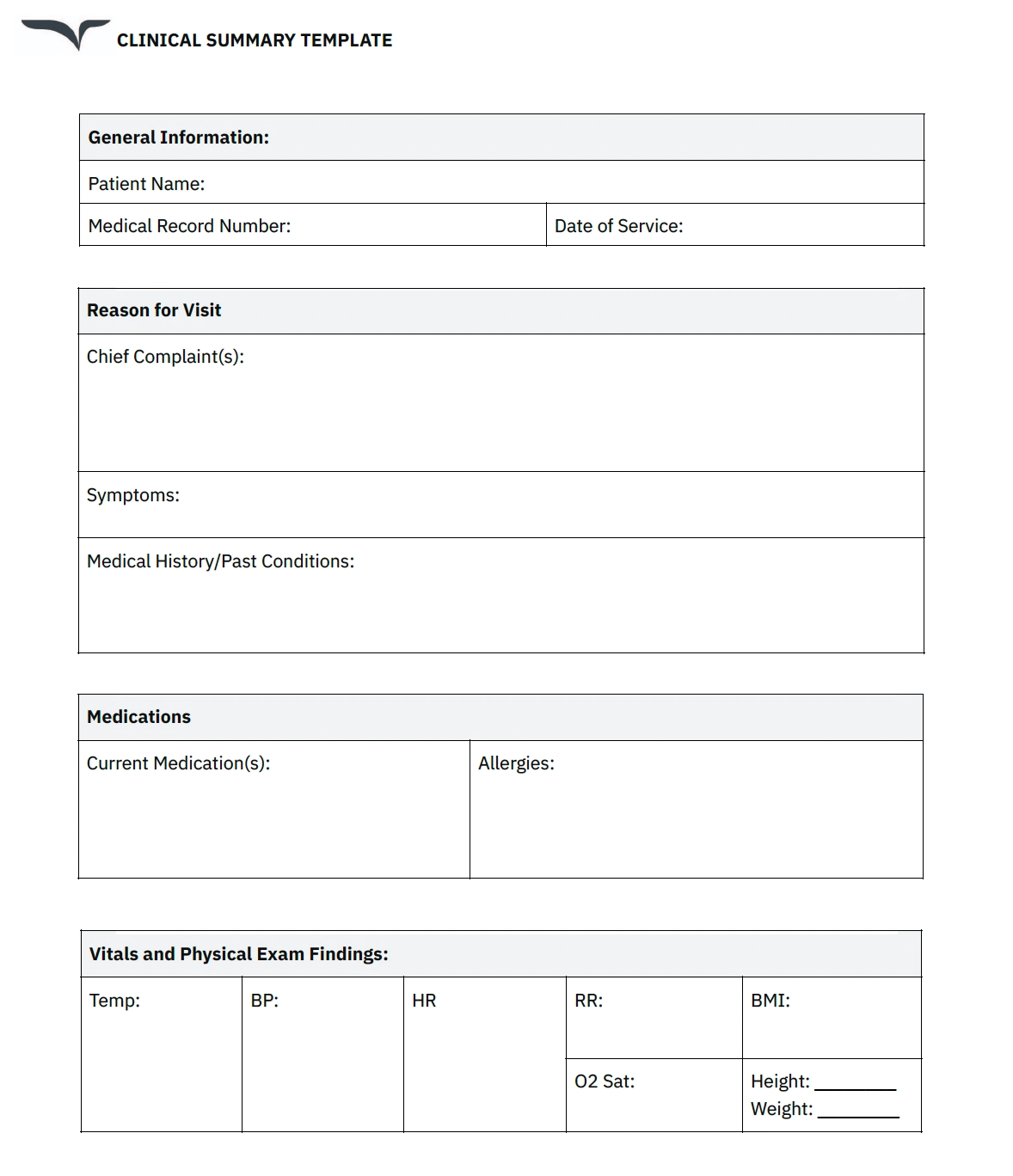
Clinical summary template
Click to download our free treatment summary template.
If you're looking for help with your clinical summary templates, you don't have to start from scratch. With Instant Templates, you can upload or paste a real note from a past visit, and Freed will turn it into a Learned Template for you, to be used again and again.
And, in the Freed template library, you'll find many templates you can choose from to add to your workflow, then tweak as needed. As you edit, Freed learns your style and helps keep your notes consistent. Get started with Freed's templates here.
Why clinical summaries matter
Clinical summaries are more than administrative paperwork. A high-quality clinical summary helps:
Improve continuity of care
A complete clinical summary ensures that every health care provider involved in treatment can quickly review the patient’s medical history, diagnosis, symptoms, treatment history, current medications, assessment findings, and treatment plan examples.
This is especially important during referrals, shift changes, discharge summary creation, and follow-up care transitions.
Reduce documentation errors
Incomplete clinical documentation increases the risk of medication errors, duplicated testing, delayed diagnosis, and inconsistent treatment recommendations.
A structured clinical summary helps standardize patient information and improve accuracy.
Support patient engagement
Patients who understand their diagnosis, treatment plan, symptoms, recommendations, and follow-up care instructions are more likely to participate in their care.
Many organizations now provide patients with a brief summary after visits so they can review their treatment recommendations, current medications, and next steps.
Strengthen legal and regulatory compliance
Clinical documentation supports billing, coding, compliance, and medical records accuracy.
A well-organized clinical summary creates a reliable record of patient progress, clinical findings, treatment decisions, and provider assessment.
Save time across the care team
When patient information is easy to review, health care providers spend less time searching through medical records and more time delivering care.
Template section breakdown: What makes up a clinical summary?
Every organization structures clinical documentation differently, but most clinical summary templates include the same core sections.
Below is a practical breakdown of the sections commonly included in a clinical summary.
1. Patient information
What to include
- Patient name
- Date of birth
- Medical record number
- Insurance information
- Visit date
- Contact information
- Primary care provider
Why it matters
Accurate patient information is the foundation of safe care.
Incorrect patient information can create serious medical records errors, treatment delays, or medication issues.
2. Presenting problem
What to include
The presenting problem explains why the patient sought care.
Examples include:
- Chest pain
- Anxiety symptoms
- Chronic knee pain
- Medication refill requests
- Depression follow-up
- New respiratory symptoms
Why it matters
The presenting problem establishes the focus of the clinical summary and guides the assessment, diagnosis, and treatment plan.
3. History of present illness (HPI)
What to include
The HPI expands on the presenting problem by documenting:
- Onset
- Location
- Duration
- Severity
- Timing
- Aggravating factors
- Relieving factors
- Associated symptoms
- Prior treatment
- Patient progress
Why it matters
A strong HPI improves diagnostic accuracy and supports clinical decision-making.
It also creates a clearer clinical summary for future follow-up care.
4. Medical history and treatment history
What to include
- Chronic conditions
- Prior diagnosis information
- Surgical history
- Family medical history
- Relevant social history
- Mental health history
- Previous treatment history
- Prior hospitalizations
Why it matters
Medical history provides critical context for the current diagnosis, assessment, symptoms, and treatment plan.
For example, a patient with diabetes, hypertension, and chronic kidney disease may require a very different treatment approach than a patient without those conditions.
In mental health settings, treatment history and prior diagnosis information are especially important for evaluating patient progress.
5. Current medications
What to include
- Medication names
- Dosages
- Frequency
- Adherence concerns
- Recent medication changes
Why it matters
Documenting current medications reduces medication interaction risks and supports safer treatment recommendations.
Current medications should always align with the treatment plan and discharge summary documentation.
6. Allergies
What to include
- Medication allergies
- Food allergies
- Reaction details
Why it matters
Accurate allergy documentation protects patient safety and reduces preventable adverse events.
7. Review of systems (ROS)
What to include
A system-by-system review of symptoms relevant to the presenting problem.
Examples include:
- Constitutional symptoms
- Respiratory symptoms
- Cardiovascular symptoms
- Gastrointestinal symptoms
- Neurological symptoms
- Mental health symptoms
Why it matters
ROS documentation helps uncover additional clinical findings that may impact diagnosis or treatment.
8. Physical examination and clinical findings
What to include
- Vital signs
- General appearance
- System-specific exam findings
- Functional status
- Behavioral observations
Why it matters
Clinical findings provide objective evidence that supports the assessment, diagnosis, and treatment plan.
Clinical findings are also critical for clinical documentation quality and medical records accuracy.
9. Assessment and diagnosis
What to include
- Primary diagnosis
- Differential diagnosis
- Severity assessment
- Risk factors
- Clinical interpretation
Why it matters
The assessment section summarizes clinical reasoning.
It connects the patient’s symptoms, medical history, clinical findings, treatment history, and presenting problem into a coherent diagnosis.
A clear assessment also improves communication between health care providers.
10. Treatment plan
What to include
- Medications
- Therapy recommendations
- Lifestyle modifications
- Specialist referrals
- Imaging or laboratory orders
- Monitoring instructions
- Follow-up care recommendations
Why it matters
The treatment plan outlines the next steps for care.
A detailed treatment plan improves patient understanding, strengthens continuity of care, and supports better patient progress.
11. Follow-up care
What to include
- Return visit timeline
- Monitoring instructions
- Escalation guidance
- Follow-up testing
- Referral coordination
Why it matters
Follow-up care instructions help patients understand what to expect after the visit.
Clear follow-up care recommendations can improve adherence, patient progress, and outcomes.
Completed clinical summary sample
Let's have a look at a specific example: a classic knee pain case.
Patient information
- Patient Name: John Doe
- Date of Birth: January 1, 1980
- Medical Record Number: 12345
- Visit Date: March 18, 2025
- Health Care Provider: Dr. Sarah Smith
Presenting problem
The patient presents with worsening left knee pain and stiffness.
History of present illness
The patient reports intermittent left knee symptoms for approximately two weeks.
Symptoms include:
- Dull aching pain
- Mild swelling
- Increased pain during weight-bearing activities
- Morning stiffness
- Reduced mobility
The patient states symptoms have gradually worsened despite conservative home treatment.
Patient progress has been limited with over-the-counter NSAIDs.
Medical history
- Hypertension
- Prior appendectomy
- No previous orthopedic surgery
- Relevant treatment history includes intermittent NSAID use
Current medications
- Lisinopril 10 mg daily
- Ibuprofen 400 mg as needed
Allergies
- Penicillin (rash)
Review of systems
- Musculoskeletal symptoms positive for knee pain and stiffness
- No chest pain
- No respiratory symptoms
- No neurological symptoms
- Mental health screening negative
Clinical findings
Vital signs stable.
Physical examination reveals:
- Mild joint effusion
- Tenderness over medial joint line
- Pain with range of motion
- Stable ligaments
Imaging demonstrates mild degenerative changes.
Assessment
Primary diagnosis:
- Mild left knee osteoarthritis
Additional assessment:
- Controlled hypertension
Treatment plan
- Initiate physical therapy
- Continue conservative treatment
- Encourage low-impact exercise
- Continue current medications as tolerated
- Weight management recommendations provided
Follow-up care
- Follow-up care visit scheduled in four weeks
- Orthopedic referral if symptoms worsen
- Monitor patient progress closely
Brief summary
The patient demonstrates mild degenerative knee disease with worsening symptoms despite conservative treatment. Current treatment plan focuses on rehabilitation, symptom management, and monitoring patient progress.
Specialty-specific clinical summary considerations
Different specialties require different approaches to clinical documentation.
Primary care
Primary care clinical summaries often include:
- Preventive care recommendations
- Chronic disease management
- Medication reconciliation
- Follow-up care coordination
- Vaccination status
Mental health
Mental health clinical summary documentation may focus more heavily on:
- Behavioral observations
- Mood assessment
- Risk assessment
- Treatment history
- Patient progress over time
- Therapy recommendations
- Mental health symptoms
Because mental health documentation may contain highly sensitive health information, clinicians should follow organizational privacy and HIPAA requirements carefully.
Urgent care
Urgent care clinical documentation often prioritizes:
- Rapid assessment
- Acute symptoms
- Immediate diagnosis
- Treatment recommendations
- Discharge summary instructions
Specialty care
Specialists may include more detailed:
- Diagnostic findings
- Procedure details
- Longitudinal patient progress
- Complex treatment history
- Advanced treatment planning
Common clinical summary challenges
Even experienced clinicians can run into clinical documentation issues.
Here are some of the most common problems:
- Incomplete patient information: Missing patient information creates risk across medical records, treatment decisions, and follow-up care.
- Overly vague assessment language: A vague assessment can reduce continuity of care and create confusion for future health care providers.
- Missing treatment history: Treatment history helps explain prior interventions, patient progress, and failed therapies.
- Poor follow-up care instructions: Patients need clear recommendations regarding medications, symptoms, monitoring, and next steps.
- Copy-and-paste documentation: Overreliance on copied clinical documentation can introduce outdated health information and inaccurate clinical findings.
Best practices for writing better clinical summaries
- Focus on clarity: A clinical summary should be easy for another health care provider to review quickly.
- Prioritize relevant information: Not every detail belongs in the summary. Focus on the most important symptoms, diagnosis details, treatment history, assessment findings, and treatment plan updates.
- Track patient progress consistently: Consistent patient progress documentation improves continuity of care and long-term treatment planning.
- Keep recommendations actionable: Recommendations should be specific and easy for patients to follow.
- Standardize your workflow: Templates and AI tools can improve consistency across clinical documentation.
AI Scribes: The future of clinical summaries?
While scanning the above example, did you notice that it could quickly become long-winded?
This is the key issue — in 2022, the average time spent generating clinical documentation increased by 25% over the last 7 years.
So, is there a solution?
AI scribes are already lightening the documentation load—no more typing marathons. Many organizations are adopting AI-powered clinical documentation tools.
AI medical scribes are virtual assistants that use artificial intelligence to document patient encounters in real time. They listen to conversations between providers and patients, analyze the information, and create accurate and comprehensive clinical summaries.
Here are a few ways AI scribes can serve as an alternative or supplement to your current system:
- Real-time documentation: Capture patient encounters in real time and generate summaries that reduce the burden of manual data entry. This not only saves time but also ensures key details are not lost.
- Increased accuracy: Accurately transcribe complex medical terminology, significantly reducing transcription errors.
- Time savings: Free up valuable time that practitioners can spend with patients — or off the clock.
- Scalability: Scale on demand without compromising the quality of documentation.
Go beyond templates
Templates are a great start, but they still rely on you doing the work.
What if you could skip the typing entirely?
Freed is an AI clinician assistant that listens, transcribes, and drafts your clinical notes — so you can focus on care, not clicks.
Try Freed free and see how fast documentation can really be.
Disclaimer: This article is for informational purposes only and does not constitute legal or clinical advice. Clinicians should follow applicable laws, regulations, and institutional policies when creating or sharing clinical documentation.
Table of Contents
77.42% of health professionals say they're finishing work later than desired. Why? Excessive documentation tasks.
Too much clinical documentation drives work after-hours, burnout, and less time with patients. NIH research on EHR burden shows that documentation tasks often spill beyond the workday. And yet, the clinical summary remains one of the most important parts of patient care.
A well-written clinical summary gives every health care provider a quick, accurate view of the patient’s medical history, presenting problem, symptoms, diagnosis, treatment history, current medications, clinical findings, patient progress, and follow-up care recommendations. It supports continuity of care, improves communication, and helps ensure every treatment plan is based on complete health information.
The challenge is that writing a comprehensive clinical summary takes time.
That’s why we created this guide.
Inside, you’ll find:
- A downloadable clinical summary template
- Examples of effective clinical documentation
- Best practices for organizing patient information
- Specialty-specific considerations
- Common mistakes to avoid
- Guidance on HIPAA-compliant AI scribes
- A real-world clinical summary example
- Tips for improving patient progress tracking and follow-up care
Whether you work in primary care, mental health, urgent care, or specialty medicine, this guide will help you create more efficient, accurate, and useful clinical summaries.
What is a clinical summary?
A clinical summary is a concise but comprehensive overview of a patient's medical history, their encounter, diagnosis, treatment, and ongoing care plan.
It captures the most important patient information from a visit and organizes it into a format that allows another health care provider to quickly understand the patient’s medical history, presenting problem, symptoms, assessment, treatment history, current medications, clinical findings, recommendations, and follow-up care plan.
A clinical summary may be used during:
- Routine office visits
- Specialist consultations
- Mental health evaluations
- Discharge summary documentation
- Transitions of care
- Emergency department visits
- Hospital admissions
- Follow-up appointments
- Referral coordination
In many organizations, the clinical summary also becomes part of the permanent medical records. Because of this, accurate clinical documentation is essential.
Clinical summary template
Click to download our free treatment summary template.
If you're looking for help with your clinical summary templates, you don't have to start from scratch. With Instant Templates, you can upload or paste a real note from a past visit, and Freed will turn it into a Learned Template for you, to be used again and again.
And, in the Freed template library, you'll find many templates you can choose from to add to your workflow, then tweak as needed. As you edit, Freed learns your style and helps keep your notes consistent. Get started with Freed's templates here.
Why clinical summaries matter
Clinical summaries are more than administrative paperwork. A high-quality clinical summary helps:
Improve continuity of care
A complete clinical summary ensures that every health care provider involved in treatment can quickly review the patient’s medical history, diagnosis, symptoms, treatment history, current medications, assessment findings, and treatment plan examples.
This is especially important during referrals, shift changes, discharge summary creation, and follow-up care transitions.
Reduce documentation errors
Incomplete clinical documentation increases the risk of medication errors, duplicated testing, delayed diagnosis, and inconsistent treatment recommendations.
A structured clinical summary helps standardize patient information and improve accuracy.
Support patient engagement
Patients who understand their diagnosis, treatment plan, symptoms, recommendations, and follow-up care instructions are more likely to participate in their care.
Many organizations now provide patients with a brief summary after visits so they can review their treatment recommendations, current medications, and next steps.
Strengthen legal and regulatory compliance
Clinical documentation supports billing, coding, compliance, and medical records accuracy.
A well-organized clinical summary creates a reliable record of patient progress, clinical findings, treatment decisions, and provider assessment.
Save time across the care team
When patient information is easy to review, health care providers spend less time searching through medical records and more time delivering care.
Template section breakdown: What makes up a clinical summary?
Every organization structures clinical documentation differently, but most clinical summary templates include the same core sections.
Below is a practical breakdown of the sections commonly included in a clinical summary.
1. Patient information
What to include
- Patient name
- Date of birth
- Medical record number
- Insurance information
- Visit date
- Contact information
- Primary care provider
Why it matters
Accurate patient information is the foundation of safe care.
Incorrect patient information can create serious medical records errors, treatment delays, or medication issues.
2. Presenting problem
What to include
The presenting problem explains why the patient sought care.
Examples include:
- Chest pain
- Anxiety symptoms
- Chronic knee pain
- Medication refill requests
- Depression follow-up
- New respiratory symptoms
Why it matters
The presenting problem establishes the focus of the clinical summary and guides the assessment, diagnosis, and treatment plan.
3. History of present illness (HPI)
What to include
The HPI expands on the presenting problem by documenting:
- Onset
- Location
- Duration
- Severity
- Timing
- Aggravating factors
- Relieving factors
- Associated symptoms
- Prior treatment
- Patient progress
Why it matters
A strong HPI improves diagnostic accuracy and supports clinical decision-making.
It also creates a clearer clinical summary for future follow-up care.
4. Medical history and treatment history
What to include
- Chronic conditions
- Prior diagnosis information
- Surgical history
- Family medical history
- Relevant social history
- Mental health history
- Previous treatment history
- Prior hospitalizations
Why it matters
Medical history provides critical context for the current diagnosis, assessment, symptoms, and treatment plan.
For example, a patient with diabetes, hypertension, and chronic kidney disease may require a very different treatment approach than a patient without those conditions.
In mental health settings, treatment history and prior diagnosis information are especially important for evaluating patient progress.
5. Current medications
What to include
- Medication names
- Dosages
- Frequency
- Adherence concerns
- Recent medication changes
Why it matters
Documenting current medications reduces medication interaction risks and supports safer treatment recommendations.
Current medications should always align with the treatment plan and discharge summary documentation.
6. Allergies
What to include
- Medication allergies
- Food allergies
- Reaction details
Why it matters
Accurate allergy documentation protects patient safety and reduces preventable adverse events.
7. Review of systems (ROS)
What to include
A system-by-system review of symptoms relevant to the presenting problem.
Examples include:
- Constitutional symptoms
- Respiratory symptoms
- Cardiovascular symptoms
- Gastrointestinal symptoms
- Neurological symptoms
- Mental health symptoms
Why it matters
ROS documentation helps uncover additional clinical findings that may impact diagnosis or treatment.
8. Physical examination and clinical findings
What to include
- Vital signs
- General appearance
- System-specific exam findings
- Functional status
- Behavioral observations
Why it matters
Clinical findings provide objective evidence that supports the assessment, diagnosis, and treatment plan.
Clinical findings are also critical for clinical documentation quality and medical records accuracy.
9. Assessment and diagnosis
What to include
- Primary diagnosis
- Differential diagnosis
- Severity assessment
- Risk factors
- Clinical interpretation
Why it matters
The assessment section summarizes clinical reasoning.
It connects the patient’s symptoms, medical history, clinical findings, treatment history, and presenting problem into a coherent diagnosis.
A clear assessment also improves communication between health care providers.
10. Treatment plan
What to include
- Medications
- Therapy recommendations
- Lifestyle modifications
- Specialist referrals
- Imaging or laboratory orders
- Monitoring instructions
- Follow-up care recommendations
Why it matters
The treatment plan outlines the next steps for care.
A detailed treatment plan improves patient understanding, strengthens continuity of care, and supports better patient progress.
11. Follow-up care
What to include
- Return visit timeline
- Monitoring instructions
- Escalation guidance
- Follow-up testing
- Referral coordination
Why it matters
Follow-up care instructions help patients understand what to expect after the visit.
Clear follow-up care recommendations can improve adherence, patient progress, and outcomes.
Completed clinical summary sample
Let's have a look at a specific example: a classic knee pain case.
Patient information
- Patient Name: John Doe
- Date of Birth: January 1, 1980
- Medical Record Number: 12345
- Visit Date: March 18, 2025
- Health Care Provider: Dr. Sarah Smith
Presenting problem
The patient presents with worsening left knee pain and stiffness.
History of present illness
The patient reports intermittent left knee symptoms for approximately two weeks.
Symptoms include:
- Dull aching pain
- Mild swelling
- Increased pain during weight-bearing activities
- Morning stiffness
- Reduced mobility
The patient states symptoms have gradually worsened despite conservative home treatment.
Patient progress has been limited with over-the-counter NSAIDs.
Medical history
- Hypertension
- Prior appendectomy
- No previous orthopedic surgery
- Relevant treatment history includes intermittent NSAID use
Current medications
- Lisinopril 10 mg daily
- Ibuprofen 400 mg as needed
Allergies
- Penicillin (rash)
Review of systems
- Musculoskeletal symptoms positive for knee pain and stiffness
- No chest pain
- No respiratory symptoms
- No neurological symptoms
- Mental health screening negative
Clinical findings
Vital signs stable.
Physical examination reveals:
- Mild joint effusion
- Tenderness over medial joint line
- Pain with range of motion
- Stable ligaments
Imaging demonstrates mild degenerative changes.
Assessment
Primary diagnosis:
- Mild left knee osteoarthritis
Additional assessment:
- Controlled hypertension
Treatment plan
- Initiate physical therapy
- Continue conservative treatment
- Encourage low-impact exercise
- Continue current medications as tolerated
- Weight management recommendations provided
Follow-up care
- Follow-up care visit scheduled in four weeks
- Orthopedic referral if symptoms worsen
- Monitor patient progress closely
Brief summary
The patient demonstrates mild degenerative knee disease with worsening symptoms despite conservative treatment. Current treatment plan focuses on rehabilitation, symptom management, and monitoring patient progress.
Specialty-specific clinical summary considerations
Different specialties require different approaches to clinical documentation.
Primary care
Primary care clinical summaries often include:
- Preventive care recommendations
- Chronic disease management
- Medication reconciliation
- Follow-up care coordination
- Vaccination status
Mental health
Mental health clinical summary documentation may focus more heavily on:
- Behavioral observations
- Mood assessment
- Risk assessment
- Treatment history
- Patient progress over time
- Therapy recommendations
- Mental health symptoms
Because mental health documentation may contain highly sensitive health information, clinicians should follow organizational privacy and HIPAA requirements carefully.
Urgent care
Urgent care clinical documentation often prioritizes:
- Rapid assessment
- Acute symptoms
- Immediate diagnosis
- Treatment recommendations
- Discharge summary instructions
Specialty care
Specialists may include more detailed:
- Diagnostic findings
- Procedure details
- Longitudinal patient progress
- Complex treatment history
- Advanced treatment planning
Common clinical summary challenges
Even experienced clinicians can run into clinical documentation issues.
Here are some of the most common problems:
- Incomplete patient information: Missing patient information creates risk across medical records, treatment decisions, and follow-up care.
- Overly vague assessment language: A vague assessment can reduce continuity of care and create confusion for future health care providers.
- Missing treatment history: Treatment history helps explain prior interventions, patient progress, and failed therapies.
- Poor follow-up care instructions: Patients need clear recommendations regarding medications, symptoms, monitoring, and next steps.
- Copy-and-paste documentation: Overreliance on copied clinical documentation can introduce outdated health information and inaccurate clinical findings.
Best practices for writing better clinical summaries
- Focus on clarity: A clinical summary should be easy for another health care provider to review quickly.
- Prioritize relevant information: Not every detail belongs in the summary. Focus on the most important symptoms, diagnosis details, treatment history, assessment findings, and treatment plan updates.
- Track patient progress consistently: Consistent patient progress documentation improves continuity of care and long-term treatment planning.
- Keep recommendations actionable: Recommendations should be specific and easy for patients to follow.
- Standardize your workflow: Templates and AI tools can improve consistency across clinical documentation.
AI Scribes: The future of clinical summaries?
While scanning the above example, did you notice that it could quickly become long-winded?
This is the key issue — in 2022, the average time spent generating clinical documentation increased by 25% over the last 7 years.
So, is there a solution?
AI scribes are already lightening the documentation load—no more typing marathons. Many organizations are adopting AI-powered clinical documentation tools.
AI medical scribes are virtual assistants that use artificial intelligence to document patient encounters in real time. They listen to conversations between providers and patients, analyze the information, and create accurate and comprehensive clinical summaries.
Here are a few ways AI scribes can serve as an alternative or supplement to your current system:
- Real-time documentation: Capture patient encounters in real time and generate summaries that reduce the burden of manual data entry. This not only saves time but also ensures key details are not lost.
- Increased accuracy: Accurately transcribe complex medical terminology, significantly reducing transcription errors.
- Time savings: Free up valuable time that practitioners can spend with patients — or off the clock.
- Scalability: Scale on demand without compromising the quality of documentation.
Go beyond templates
Templates are a great start, but they still rely on you doing the work.
What if you could skip the typing entirely?
Freed is an AI clinician assistant that listens, transcribes, and drafts your clinical notes — so you can focus on care, not clicks.
Try Freed free and see how fast documentation can really be.
Disclaimer: This article is for informational purposes only and does not constitute legal or clinical advice. Clinicians should follow applicable laws, regulations, and institutional policies when creating or sharing clinical documentation.
FAQs
Frequently asked questions from clinicians and medical practitioners.
How do you write a good clinical summary?
What is the difference between a clinical overview and a clinical summary?

Related content
Free yourself for better things
548 Market Street, PMB 95301
San Francisco, CA 94104
Specialties
Compliance & Security
Our technology is HIPAA-compliant, uses industry best practices, and doesn’t store patient recordings.