Psychotherapy Note Template: Examples, HIPAA, and Best Practices
Psychotherapy notes are often misunderstood in mental health documentation. For a health care provider working in mental health, psychotherapy notes are not just documentation—they are a private clinical thinking space used to document or analyze the contents of conversation during a private counseling session, group counseling session, or family counseling session.
Unlike a medical record, psychotherapy notes are intentionally kept separate from the rest of the clinical system and protected under HIPAA.
For many mental health professionals, psychotherapy notes serve as a higher level of confidentiality—supporting reflection, hypothesis-building, and clinical reasoning without becoming part of the formal medical record.
This guide breaks down:
- How psychotherapy notes work
- How they differ from a medical record
- How to structure them effectively using a psychotherapy note template designed for real-world clinical workflows
What is a psychotherapy note?
Psychotherapy notes are a clinician’s personal observations and analyses during therapy sessions.
Think of them as your internal monologue during sessions, minus the background noise and awkward silences.
Psychotherapy notes are:
- Private: For your eyes only. Not part of the official medical record.
- Reflective: They capture your impressions, emotional reactions, hunches, and maybe that odd feeling you got during the client’s story about their cat.
- Flexible: There’s no required format, just your thoughts flowing in a way that makes sense to you.
Why bother? Because our brains aren’t filing cabinets. If you want to remember that tiny detail from week 3 that suddenly makes sense in week 9, you’ll want these notes around. Psychotherapy notes are personal notes created by a mental health professional during or after a counseling session to document or analyze the contents of conversation.
Psychotherapy notes are used by a health care provider to reflect on:
- Symptoms presented by a patient during a counseling session
- Diagnosis impressions and clinical interpretation
- Treatment direction and treatment plan considerations
- Prognosis and progress to date
- Functional status of the patient
- Clinical tests discussed or interpreted during care
Psychotherapy notes are not part of the medical record and are explicitly excluded information under HIPAA when properly designated. A psychotherapy note is separate from the rest of the documentation workflow and is designed to remain separate from the rest of the clinical system.
Free psychotherapy note template
When your thoughts are moving fast between sessions, structure is your safety net. Our psychotherapy note template helps you stay grounded — without slowing you down.
That’s why we created a psychotherapy note template to make life easier for you.
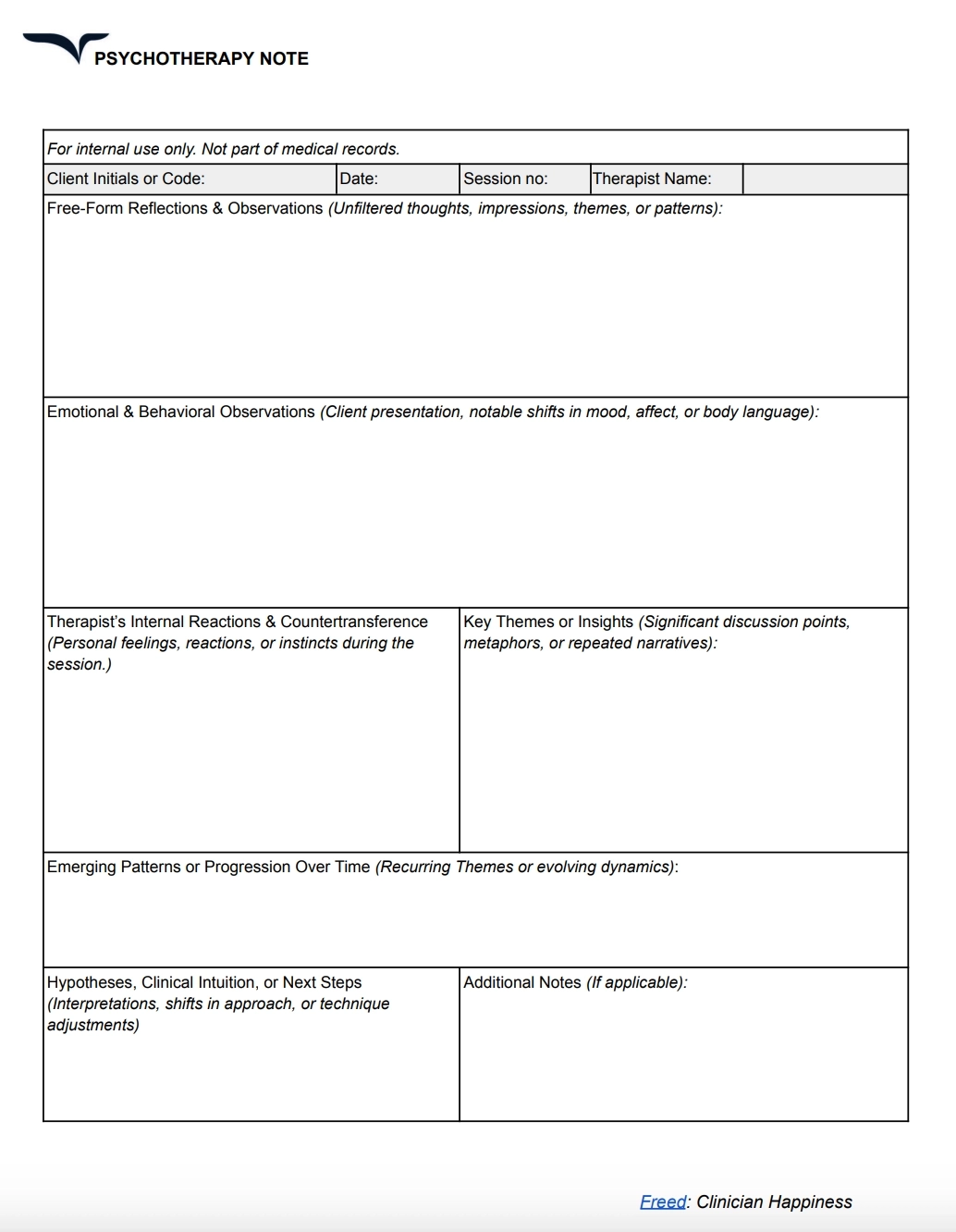
📌 Download free psychotherapy note template
Streamline documentation with reusable psychotherapy note templates
Easily transform your existing patient intake forms into templates within Freed. Upload a sample note, and Freed reviews its structure, formatting, and content to build a template for future use. You can also choose from a wide range of prebuilt options in Freed’s template library.
As you refine your notes, Freed continuously updates your templates to better reflect your preferred workflow. Discover how Freed templates can simplify and standardize your note-taking.
Why psychotherapy notes exist
Psychotherapy notes exist because mental health treatment requires cognitive space for reflection.
During a counseling session, a mental health professional may observe:
- Emotional responses from the patient
- Subtle symptom shifts
- Changes in prognosis or engagement
- Functional status fluctuations
- Treatment resistance or alignment
These observations may not belong in the medical record but are essential for clinical reasoning. Psychotherapy notes allow a health care provider to document or analyze the contents of conversation without turning every reflection into formal documentation.
What goes into psychotherapy notes?
Psychotherapy notes are designed to document or analyze the contents of conversation in a way that supports clinical reasoning.
A strong psychotherapy note template includes:
1. Counseling session details
- Private counseling session, group counseling session, or family counseling session
- Start and stop times
- Frequencies of treatment
- Health care provider identification
2. Clinical observations
- Symptoms presented by the patient
- Behavioral changes during treatment
- Functional status updates
- Clinical tests or informal assessments
3. Clinical interpretation
- Diagnosis impressions
- Prognosis considerations
- Treatment direction hypotheses
- Treatment plan reflections
4. Provider reflection
- Mental health professional observations
- Clinical intuition
- Document or analyze patterns in behavior or emotion
5. Progress tracking
- Progress to date
- Changes across counseling session history
- Response to treatment
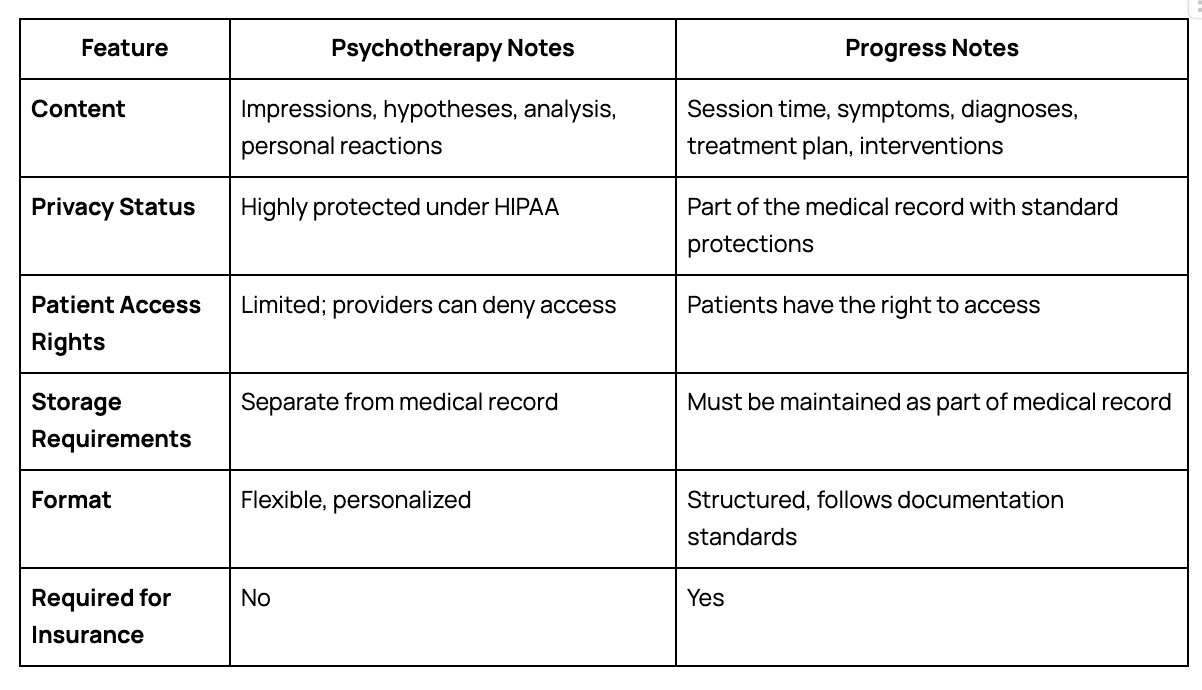
Psychotherapy notes vs. medical record documentation
A key distinction every mental health professional must understand is the difference between psychotherapy notes and the medical record.
A medical record may include:
- Diagnosis and diagnosis updates
- Treatment plan and treatment progress
- Medication prescription information
- Symptoms and functional status
- Start and stop times of treatment
- Frequencies of treatment sessions
- Clinical tests and results
- Progress to date
- Prognosis and care planning
By contrast, psychotherapy notes are intentionally excluded information and are not part of the medical record.
Psychotherapy notes document or analyze the contents of conversation during a private counseling session and are kept separate from the rest of the patient chart.
This separation is critical for HIPAA compliance and the privacy rule governing protected health information.
Here’s a preview of how psychotherapy notes compare against regular medical progress notes:
HIPAA and psychotherapy notes compliance
Under HIPAA, psychotherapy notes are given special protection and a higher level of confidentiality and security compared to the medical record.
Psychotherapy notes require:
- Authorization required before disclosure in most cases
- Strict separation from the rest of the medical record
- Protected storage as excluded information
- Limited use or disclosure exceptions
HIPAA defines psychotherapy notes as separate designation documentation that is not part of routine treatment, payment, or health care operations unless specific authorization is provided.
Disclosure of psychotherapy notes typically requires patient authorization, except in narrow legal exceptions.
Clinicians need space to process complex emotions and document their own observations without compromising patient privacy or stressing about external reviews. That’s where psychotherapy notes come in handy.
And finally, psychotherapy notes have an additional layer of legal protection with more than usual steps to access these documents. This protects the patient and provider’s privacy in case of lawsuits.
Psychotherapy notes in real clinical workflows
In real-world mental health treatment, psychotherapy notes support multiple care environments:
- Private counseling session: Psychotherapy notes capture internal reflections about symptoms, diagnosis evolution, and treatment response.
- Group counseling session: Psychotherapy notes may document interpersonal dynamics, functional status changes, and group-level treatment observations.
- Family counseling session: Psychotherapy notes often include relational patterns, prognosis considerations, and treatment plan adjustments.
Across all settings, psychotherapy notes help a mental health professional document or analyze the contents of conversation without impacting the formal medical record.
Common compliance mistakes
Health care providers often unintentionally compromise psychotherapy notes separation by:
- Mixing psychotherapy notes into the medical record
- Failing to maintain separate designation storage
- Including medication prescription details in psychotherapy notes
- Documenting treatment plan elements in psychotherapy notes
- Not clearly separating excluded information
Psychotherapy notes guidelines
Even though psychotherapy notes aren’t a part of mental health records, clinicians still have to follow a few crucial guidelines when preparing these notes. Let’s break them down.
Physically separate your notes
Keep psychotherapy notes physically away from other paperwork.
Whether it's pen and paper or a digital file, store these notes separately from all other progress notes.
This is a legal requirement under HIPAA for maintaining special protections.
Use professional language
While these are private notes, maintain professional language to avoid any judgmental or problematic statements.
These notes can be audited in the future in case of legal proceedings. Meet professionalism standards and maintain a patient’s privacy.
Cover relevant insights
Psychotherapy notes focus on your personal reflections and hypotheses about a patient. You can also use this space to discuss your therapeutic process.
They don't require medical information about session timing, medication, treatment plans, and more. Maintain clear boundaries between the two types of notes (official and private) to avoid any overlap.
Plan retention policies
As a best practice, a healthcare provider should eventually delete psychotherapy notes.
You can destroy these notes once they're outdated and no longer serve a clinical purpose.
Remember to be consistent with your retention policy so you don't delete any notes for an ongoing patient.
Progress tracking using psychotherapy notes
Psychotherapy notes are especially valuable for tracking:
- Progress to date
- Shifts in symptoms
- Functional status improvements or declines
- Changes in prognosis
- Evolving diagnosis impressions
Because psychotherapy notes document or analyze the contents of conversation over time, they help a mental health professional refine treatment planning.
Treatment planning and psychotherapy notes
While psychotherapy notes are not part of the formal treatment plan, they heavily influence it. A health care provider may use psychotherapy notes to refine:
- Treatment plan adjustments
- Therapy modalities
- Session frequencies of treatment
- Clinical focus areas
Psychotherapy notes remain separate from the rest of the medical record but directly support clinical decision-making.
A new approach: Sharing psychotherapy notes with patients
Mental health clinicians are asking:What if patients could see what we see?
Research suggests that sharing psychotherapy notes could build trust and deepen engagement—if done with care.Patients have easy access to progress notes. But psychotherapy notes have traditionally remained for your eyes only.
So, why is this shift happening, and what does it mean for the future of mental healthcare?
The landscape shift toward patient autonomy
A research study evaluated the prospect of sharing psychotherapy notes with patients to maximize transpinarency in a healthcare setting.
This study advocates for patient autonomy, which means that patients have a complete understanding of their care. While clinicians agree that sharing these notes can lead to some degree of confusion, many believe that this exercise can empower patients to make health-related decisions.
The study notes:
“By signaling trust in the patient as a “grown-up” care partner, and by facilitating greater time to reflect on disclosures, open notes may strengthen patients' sense of agency and can conceivably play a role in improving outcomes.”
A key argument in favor of sharing these notes is the chance to gain patients’ trust and involve them more deeply in the care delivery process.
Let’s understand how this process can harm or benefit both parties involved.
Key challenges with sharing psychotherapy notes
Shared psychotherapy notes with patients have their barriers. How can you be candid?
This might lead to an endless list of psychotherapy notes: one for personal use and another for sharing.
Your thoughts can also be confusing when patients don’t have enough context. This step can potentially disrupt the therapy session by creating distress or doubt among patients.
Benefits of sharing psychotherapy notes with patients
In short: transparency strengthens relationships.
Patients can gain a clear insight into their therapist’s perspective and clinical thought process. It can strengthen trust between the two parties.
Besides, access to these notes would also make patients feel more invested in the process. They’ll have a tangible understanding of their emotions, patterns, and behaviors. This is equally important for maintaining continuity between sessions where patients can review discussions from the previous one.
And lastly, sharing these notes allows patients to pinpoint any misunderstandings or incorrect interpretations. They can offer more context to clear the air around any subject.
Final thoughts
So where does that leave us?
Therapy is built on trust. But trust doesn’t mean giving up your clinical space. The future won’t be all or nothing. It will be nuanced —because care is nuanced.
Clinicians need room to think clearly and candidly. Patients want to feel seen and trusted. Both can be true.
What’s next isn’t about choosing sides. It’s about creating tools and practices that protect what’s personal, while making space for connection when it matters most.
Documentation should support your thinking, versus reshape it.
Ready to streamline your psychotherapy notes?
Freed helps mental health professionals create psychotherapy notes that stay separate from the medical record, reduce documentation friction, and keep your clinical reasoning organized across every counseling session.
Try Freed for free and see how much easier psychotherapy notes can feel in your day-to-day workflow.
Disclaimer: This article is for informational purposes only and does not constitute legal or clinical advice. Clinicians should follow applicable laws, regulations, and institutional policies when creating or sharing psychotherapy notes.
Psychotherapy Note Template: Examples, HIPAA, and Best Practices
Table of Contents
Psychotherapy notes are often misunderstood in mental health documentation. For a health care provider working in mental health, psychotherapy notes are not just documentation—they are a private clinical thinking space used to document or analyze the contents of conversation during a private counseling session, group counseling session, or family counseling session.
Unlike a medical record, psychotherapy notes are intentionally kept separate from the rest of the clinical system and protected under HIPAA.
For many mental health professionals, psychotherapy notes serve as a higher level of confidentiality—supporting reflection, hypothesis-building, and clinical reasoning without becoming part of the formal medical record.
This guide breaks down:
- How psychotherapy notes work
- How they differ from a medical record
- How to structure them effectively using a psychotherapy note template designed for real-world clinical workflows
What is a psychotherapy note?
Psychotherapy notes are a clinician’s personal observations and analyses during therapy sessions.
Think of them as your internal monologue during sessions, minus the background noise and awkward silences.
Psychotherapy notes are:
- Private: For your eyes only. Not part of the official medical record.
- Reflective: They capture your impressions, emotional reactions, hunches, and maybe that odd feeling you got during the client’s story about their cat.
- Flexible: There’s no required format, just your thoughts flowing in a way that makes sense to you.
Why bother? Because our brains aren’t filing cabinets. If you want to remember that tiny detail from week 3 that suddenly makes sense in week 9, you’ll want these notes around. Psychotherapy notes are personal notes created by a mental health professional during or after a counseling session to document or analyze the contents of conversation.
Psychotherapy notes are used by a health care provider to reflect on:
- Symptoms presented by a patient during a counseling session
- Diagnosis impressions and clinical interpretation
- Treatment direction and treatment plan considerations
- Prognosis and progress to date
- Functional status of the patient
- Clinical tests discussed or interpreted during care
Psychotherapy notes are not part of the medical record and are explicitly excluded information under HIPAA when properly designated. A psychotherapy note is separate from the rest of the documentation workflow and is designed to remain separate from the rest of the clinical system.
Free psychotherapy note template
When your thoughts are moving fast between sessions, structure is your safety net. Our psychotherapy note template helps you stay grounded — without slowing you down.
That’s why we created a psychotherapy note template to make life easier for you.
📌 Download free psychotherapy note template
Streamline documentation with reusable psychotherapy note templates
Easily transform your existing patient intake forms into templates within Freed. Upload a sample note, and Freed reviews its structure, formatting, and content to build a template for future use. You can also choose from a wide range of prebuilt options in Freed’s template library.
As you refine your notes, Freed continuously updates your templates to better reflect your preferred workflow. Discover how Freed templates can simplify and standardize your note-taking.
Why psychotherapy notes exist
Psychotherapy notes exist because mental health treatment requires cognitive space for reflection.
During a counseling session, a mental health professional may observe:
- Emotional responses from the patient
- Subtle symptom shifts
- Changes in prognosis or engagement
- Functional status fluctuations
- Treatment resistance or alignment
These observations may not belong in the medical record but are essential for clinical reasoning. Psychotherapy notes allow a health care provider to document or analyze the contents of conversation without turning every reflection into formal documentation.
What goes into psychotherapy notes?
Psychotherapy notes are designed to document or analyze the contents of conversation in a way that supports clinical reasoning.
A strong psychotherapy note template includes:
1. Counseling session details
- Private counseling session, group counseling session, or family counseling session
- Start and stop times
- Frequencies of treatment
- Health care provider identification
2. Clinical observations
- Symptoms presented by the patient
- Behavioral changes during treatment
- Functional status updates
- Clinical tests or informal assessments
3. Clinical interpretation
- Diagnosis impressions
- Prognosis considerations
- Treatment direction hypotheses
- Treatment plan reflections
4. Provider reflection
- Mental health professional observations
- Clinical intuition
- Document or analyze patterns in behavior or emotion
5. Progress tracking
- Progress to date
- Changes across counseling session history
- Response to treatment
Psychotherapy notes vs. medical record documentation
A key distinction every mental health professional must understand is the difference between psychotherapy notes and the medical record.
A medical record may include:
- Diagnosis and diagnosis updates
- Treatment plan and treatment progress
- Medication prescription information
- Symptoms and functional status
- Start and stop times of treatment
- Frequencies of treatment sessions
- Clinical tests and results
- Progress to date
- Prognosis and care planning
By contrast, psychotherapy notes are intentionally excluded information and are not part of the medical record.
Psychotherapy notes document or analyze the contents of conversation during a private counseling session and are kept separate from the rest of the patient chart.
This separation is critical for HIPAA compliance and the privacy rule governing protected health information.
Here’s a preview of how psychotherapy notes compare against regular medical progress notes:
HIPAA and psychotherapy notes compliance
Under HIPAA, psychotherapy notes are given special protection and a higher level of confidentiality and security compared to the medical record.
Psychotherapy notes require:
- Authorization required before disclosure in most cases
- Strict separation from the rest of the medical record
- Protected storage as excluded information
- Limited use or disclosure exceptions
HIPAA defines psychotherapy notes as separate designation documentation that is not part of routine treatment, payment, or health care operations unless specific authorization is provided.
Disclosure of psychotherapy notes typically requires patient authorization, except in narrow legal exceptions.
Clinicians need space to process complex emotions and document their own observations without compromising patient privacy or stressing about external reviews. That’s where psychotherapy notes come in handy.
And finally, psychotherapy notes have an additional layer of legal protection with more than usual steps to access these documents. This protects the patient and provider’s privacy in case of lawsuits.
Psychotherapy notes in real clinical workflows
In real-world mental health treatment, psychotherapy notes support multiple care environments:
- Private counseling session: Psychotherapy notes capture internal reflections about symptoms, diagnosis evolution, and treatment response.
- Group counseling session: Psychotherapy notes may document interpersonal dynamics, functional status changes, and group-level treatment observations.
- Family counseling session: Psychotherapy notes often include relational patterns, prognosis considerations, and treatment plan adjustments.
Across all settings, psychotherapy notes help a mental health professional document or analyze the contents of conversation without impacting the formal medical record.
Common compliance mistakes
Health care providers often unintentionally compromise psychotherapy notes separation by:
- Mixing psychotherapy notes into the medical record
- Failing to maintain separate designation storage
- Including medication prescription details in psychotherapy notes
- Documenting treatment plan elements in psychotherapy notes
- Not clearly separating excluded information
Psychotherapy notes guidelines
Even though psychotherapy notes aren’t a part of mental health records, clinicians still have to follow a few crucial guidelines when preparing these notes. Let’s break them down.
Physically separate your notes
Keep psychotherapy notes physically away from other paperwork.
Whether it's pen and paper or a digital file, store these notes separately from all other progress notes.
This is a legal requirement under HIPAA for maintaining special protections.
Use professional language
While these are private notes, maintain professional language to avoid any judgmental or problematic statements.
These notes can be audited in the future in case of legal proceedings. Meet professionalism standards and maintain a patient’s privacy.
Cover relevant insights
Psychotherapy notes focus on your personal reflections and hypotheses about a patient. You can also use this space to discuss your therapeutic process.
They don't require medical information about session timing, medication, treatment plans, and more. Maintain clear boundaries between the two types of notes (official and private) to avoid any overlap.
Plan retention policies
As a best practice, a healthcare provider should eventually delete psychotherapy notes.
You can destroy these notes once they're outdated and no longer serve a clinical purpose.
Remember to be consistent with your retention policy so you don't delete any notes for an ongoing patient.
Progress tracking using psychotherapy notes
Psychotherapy notes are especially valuable for tracking:
- Progress to date
- Shifts in symptoms
- Functional status improvements or declines
- Changes in prognosis
- Evolving diagnosis impressions
Because psychotherapy notes document or analyze the contents of conversation over time, they help a mental health professional refine treatment planning.
Treatment planning and psychotherapy notes
While psychotherapy notes are not part of the formal treatment plan, they heavily influence it. A health care provider may use psychotherapy notes to refine:
- Treatment plan adjustments
- Therapy modalities
- Session frequencies of treatment
- Clinical focus areas
Psychotherapy notes remain separate from the rest of the medical record but directly support clinical decision-making.
A new approach: Sharing psychotherapy notes with patients
Mental health clinicians are asking:What if patients could see what we see?
Research suggests that sharing psychotherapy notes could build trust and deepen engagement—if done with care.Patients have easy access to progress notes. But psychotherapy notes have traditionally remained for your eyes only.
So, why is this shift happening, and what does it mean for the future of mental healthcare?
The landscape shift toward patient autonomy
A research study evaluated the prospect of sharing psychotherapy notes with patients to maximize transpinarency in a healthcare setting.
This study advocates for patient autonomy, which means that patients have a complete understanding of their care. While clinicians agree that sharing these notes can lead to some degree of confusion, many believe that this exercise can empower patients to make health-related decisions.
The study notes:
“By signaling trust in the patient as a “grown-up” care partner, and by facilitating greater time to reflect on disclosures, open notes may strengthen patients' sense of agency and can conceivably play a role in improving outcomes.”
A key argument in favor of sharing these notes is the chance to gain patients’ trust and involve them more deeply in the care delivery process.
Let’s understand how this process can harm or benefit both parties involved.
Key challenges with sharing psychotherapy notes
Shared psychotherapy notes with patients have their barriers. How can you be candid?
This might lead to an endless list of psychotherapy notes: one for personal use and another for sharing.
Your thoughts can also be confusing when patients don’t have enough context. This step can potentially disrupt the therapy session by creating distress or doubt among patients.
Benefits of sharing psychotherapy notes with patients
In short: transparency strengthens relationships.
Patients can gain a clear insight into their therapist’s perspective and clinical thought process. It can strengthen trust between the two parties.
Besides, access to these notes would also make patients feel more invested in the process. They’ll have a tangible understanding of their emotions, patterns, and behaviors. This is equally important for maintaining continuity between sessions where patients can review discussions from the previous one.
And lastly, sharing these notes allows patients to pinpoint any misunderstandings or incorrect interpretations. They can offer more context to clear the air around any subject.
Final thoughts
So where does that leave us?
Therapy is built on trust. But trust doesn’t mean giving up your clinical space. The future won’t be all or nothing. It will be nuanced —because care is nuanced.
Clinicians need room to think clearly and candidly. Patients want to feel seen and trusted. Both can be true.
What’s next isn’t about choosing sides. It’s about creating tools and practices that protect what’s personal, while making space for connection when it matters most.
Documentation should support your thinking, versus reshape it.
Ready to streamline your psychotherapy notes?
Freed helps mental health professionals create psychotherapy notes that stay separate from the medical record, reduce documentation friction, and keep your clinical reasoning organized across every counseling session.
Try Freed for free and see how much easier psychotherapy notes can feel in your day-to-day workflow.
Disclaimer: This article is for informational purposes only and does not constitute legal or clinical advice. Clinicians should follow applicable laws, regulations, and institutional policies when creating or sharing psychotherapy notes.
FAQs
Frequently asked questions from clinicians and medical practitioners.
What is considered a psychotherapy note?
What is the difference between a therapy note and a progress note?
How do you document psychotherapy notes?
Can therapist notes be used as evidence?
What does HIPAA say about psychotherapy notes?
Are psychotherapy notes required?
Are psychotherapy notes part of the medical record?

Related content
Free yourself for better things
548 Market Street, PMB 95301
San Francisco, CA 94104
Specialties
Compliance & Security
Our technology is HIPAA-compliant, uses industry best practices, and doesn’t store patient recordings.