What are Medical Charts? Examples & Best Practices
If you listen closely in a clinic after hours, you might hear the quiet tapping of keyboards long after the last patient has gone home. A physician finishing charting. A nurse completing progress notes. A clinician double-checking patient information before signing off.
For many clinicians, medical charting is the invisible half of patient care. It’s the work that happens after the exam, after the diagnosis, and often after the shift.
Done well, charting ensures continuity of care, supports clinical decision making, and protects clinicians through proper legal documentation. Done poorly—or delayed—it increases risk, disrupts continuity and communication, and adds to the growing documentation burden across modern healthcare.
This article explores the past, present, and future of medical charting — from paper records to an AI scribe for medical charting — and how smarter tools may finally make patient charting easier for clinicians.
What is a medical chart?
Medical charting is the process of recording patient information, clinical observations, diagnoses, and treatments in a patient record. This documentation forms the backbone of modern healthcare.
At its core, patient charting tells the story of a patient’s care. Clinicians use charting to record patient history, treatments, and decisions made during encounters.
Dr. Jill Moes writes in Op-Med that medical charts are how she holds onto the human side of medicine in a sea of demands.
“Rather than just a rote history of clinical data, they can in fact be a detailed record of who my patient is and what really matters to them.” — Dr. Jill Moes
The components of a patient's medical chart include:
- Individual patient demographics
- Medication administration
- Medical history
- Treatment plan
- Test results
- Informed consent
- Progress notes
- Referral notes
- Patient narratives
Each element contributes to accurate documentation that helps clinicians understand the patient’s current condition and previous care. Without consistent medical charting, critical patient information can be lost, which undermines continuity of care and complicates clinical decision making.
Why medical charts are crucial in patient care
Imagine a patient arriving at the emergency department with a severe allergic reaction.
Without a medical chart, every doctor’s visit is a guessing game. The care team may not know the patient’s allergy history, medications, or previous reactions. Good charting prevents these dangerous knowledge gaps. Effective medical charting supports several core functions in healthcare:
1. Continuity of care
Clinicians rely on charting to maintain continuity of care across providers, departments, and facilities. Clear patient charting ensures that the next clinician can quickly understand what has happened and what should happen next.
Well-organized chart sections allow clinicians to quickly locate patient information, review progress notes, and assess treatment outcomes. This supports strong continuity and communication between care teams.
3. Legal compliance and risk management
Medical records also serve as legal documentation. Detailed patient charting protects clinicians and organizations through proper legal compliance and risk management.
Courts and regulators often rely on accurate documentation to evaluate whether appropriate care was delivered. According to one Harvard study, 20% of medical malpractice cases involve at least one documentation failure.
Poor or missing charting can expose clinicians to liability. For that reason, timely documentation and clear and concise language are considered essential best practices in modern healthcare.
A brief history of medical charts
Humans have recorded injuries and illnesses for thousands of years. Over 15,000 years ago, humans documented injuries (likely from an animal attack) on cave walls.
These primitive records were early attempts at charting—a way to document patient information and track outcomes. Over time, physicians began recording more detailed, formalized patient history and treatments with more objective language.
Paper charts: The start of systematic records
Paper charts, notorious for their unreadable handwriting, were the gold standard from the 1800s to the late 20th century.
They were simple, cost-effective, and immune to cyberattacks, but they had major downsides: storage was a nightmare, they got lost easily, and deciphering notes sometimes felt like cracking an ancient code.
Despite these issues, paper charting allowed clinicians to document care using clear and concise language. As Dr. Woojin Joo put it in his newsletter, they reminded him that patient care only requires three things: clinical knowledge, a pen, and paper.
The rise of electronic health records: Secure documentation at scale
The transition to digital records marked a major shift in medical charting. The EHR (electronic health record) allowed organizations to store and share large volumes of patient information across systems.
EHRs introduced standardized chart sections, searchable documentation, and digital patient charting tools. By the 90s, many hospitals had EHRs. By 2009, they were mandated.
Adoption skyrocketed, growing eight-fold in six years, with 90% of hospitals and 80% of physicians now using them for the medical record.
Data-driven health: Intuitive, user-friendly charts
Today, EHRs helped clinicians make medical charting work for scaled systems — but AI, big data, and automation are helping clinicians make medical charts work for them.
Instead of simply digitizing records, these technologies analyze information, actively assist in document creation, and even anticipate needs. These include:
- AI medical note tools that listen to patient visits and automatically generate clinical notes.
- Machine learning algorithms that detect early signs of disease from medical records.
- Speech-to-text AI that enables hands-free charting.
- Cloud-based platforms that break down data silos for seamless sharing across medical records.
Challenges of modern medical charts
While the EHR (electronic health record) improved access to patient information, it also increased the documentation burden placed on clinicians. The modern documentation burden in healthcare comes from several factors:
- Complex billing requirements
- Regulatory legal compliance
- Detailed legal documentation
- Administrative reporting
Clinicians report spending half their day on documentation, multi-tasking between patient and computer.
“There are patients who feel that their health care providers aren’t able to pay full attention to the patients themselves because the doctor is consumed by this technology,” — Dr. Steven Stack, AMA, US News.
Common challenges include:
EHR usability and clinician burnout
In many systems, simple charting tasks require multiple steps. Checking lab results may take several clicks. Updating medication administration requires navigating multiple tabs. Even locating key patient information inside the EHR can take longer than expected.
These small inefficiencies quickly compound. Over the course of a day, clinicians may spend hours navigating the EHR just to complete routine documentation. One study by Mayo Clinic found that the loss of control clinicians feel from poor EHR usability is one of the biggest contributors to burnout.
Documentation overload
Many clinicians feel pressure to produce extensive patient charting in order to meet billing requirements, support legal compliance, and maintain accurate documentation.
When clinicians rush through medical charting at the end of the day, they may resort to copying and pasting text between chart sections or writing excessively detailed progress notes. This type of documentation often buries the most important clinical insights and makes it harder for other providers to quickly review patient information.The result is longer notes and less clarity.
Interoperability challenges
Another major challenge in patient charting is the lack of interoperability between systems. When different organizations use incompatible platforms, continuity and communication suffer.
Clinicians may need to manually re-enter documentation or request records from other providers.
Without better interoperability, medical charting becomes fragmented across systems instead of supporting the coordinated healthcare patients need.
Best practices for effective medical charting
Improving patient charting does not always require new technology. Many improvements come from following proven best practices.
1. Use clear and concise language
One of the most important best practices in medical charting is using clear and concise language. Notes should focus on relevant clinical facts and avoid unnecessary detail. Write notes with the goal of making it easier for patients and/or other clinicians to understand.
2. Maintain objectivity
Clinicians should always use objective language when writing progress notes. Avoid subjective statements. Instead, focus on measurable observations. For example:
- Poor charting: “Patient seems uncomfortable.”
- Better charting: “Patient reports pain level of 7/10.”
Consistent objective language improves accurate documentation and strengthens legal documentation.
3. Record vital signs consistently
Clinicians should record vital signs during every appropriate encounter. Proper charting of vitals supports clinical decision making and helps identify trends. Typical vitals to record vital signs include:
- Blood pressure
- Heart rate
- Temperature
- Respiratory rate
Failure to record vital signs can create gaps in patient charting.
4. Document in real time (or as close as possible)
Whenever feasible, complete documentation during or immediately after the encounter rather than at the end of the day. You may want to use an ambient listening aide to help capture notes simultaneously while you conduct patient visits. This reduces omissions, improves accuracy, and creates a clearer temporal record of what happened when, which is useful both for clinical handoffs and in any future legal review.
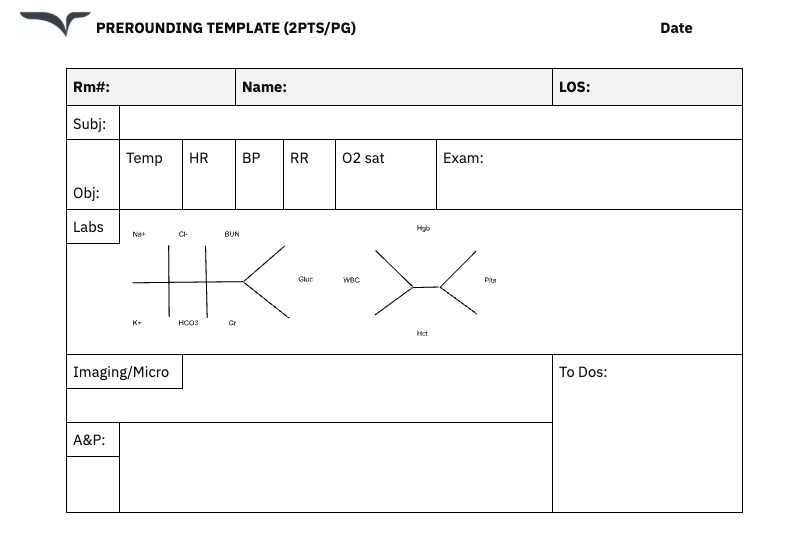
SOAP charting: A common clinical format
One of the most widely used formats for patient charting is SOAP charting. SOAP charting structures clinical notes into four parts:
- Subjective
- Objective
- Assessment
- Plan
Clinicians rely on SOAP charting because it promotes organized chart sections and consistent documentation.
For example:
- Subjective: Patient reports symptoms and relevant patient history.
- Objective: Clinician observations, including record vital signs and exam findings.
- Assessment: Diagnosis and interpretation supporting clinical decision making.
- Plan: Treatment plan, follow-up care, and medication administration.
Many clinicians prefer SOAP charting because it improves continuity of care and supports accurate documentation.
How AI is transforming charting
AI is changing charting from a manual, click-heavy task into a more automated, conversational workflow. The table below highlights concrete ways AI tools reshape documentation and why those changes matter at the point of care.
The future of medical charts
We’ve seen how far medical charts have come — but there’s a long way to go.
From AI-led workflow enhancements to voice-assisted documentation, and better interoperability, this new wave of technology is bridging the user experience gaps that have made digital charting so cumbersome for clinicians.
- AI medical scribes: AI scribes like Freed turn patient conversations into structured notes—so clinicians can finish charts faster."
- Interoperability solutions: New frameworks help EHRs talk to each other—so clinicians don’t waste time on manual work
- AI chart audits: Platforms like SmarterDx help hospitals automatically scan medical records for documentation gaps before insurance claims are submitted. This helps CDI as hospitals address issues before it impacts revenue or compliance.
- Automated medical coding: This technology uses AI to convert physician notes into standardized diagnostic codes. It reduces errors and relieves clinicians of the burden of entering codes.
Smarter tech that helps clinicians do simple things better
For generations, clinicians have relied on charting to capture the story of patient care. From handwritten notes to the modern EHR, the goal of medical charting has always been the same: document patient information clearly enough to support treatment, enable clinical decision making, and ensure continuity of care.
The transition from paper charts to EHRs had its weaknesses, but that experience taught us that technology is only as good as its usability.
The next wave of innovation is about removing the busywork EHRs created.
These new tools are here to make medical charts more intuitive and human-centered, not to make clinicians feel like they have to learn another system.
Spend less time charting with Freed
Freed was built around a simple idea: clinicians shouldn’t have to choose between great patient care and finishing their notes.
Freed listens during patient visits and automatically generates structured clinical notes, so you can walk out of the room with documentation already drafted and ready to review. No late-night charting. No scrambling to remember details hours later.
Clinicians use Freed to:
- Finish notes dramatically faster
- Stay fully present during patient conversations
- Reduce after-hours documentation
- Produce consistent, high-quality notes with minimal effort
The result is simple: less time typing, more time practicing medicine.
Table of Contents
If you listen closely in a clinic after hours, you might hear the quiet tapping of keyboards long after the last patient has gone home. A physician finishing charting. A nurse completing progress notes. A clinician double-checking patient information before signing off.
For many clinicians, medical charting is the invisible half of patient care. It’s the work that happens after the exam, after the diagnosis, and often after the shift.
Done well, charting ensures continuity of care, supports clinical decision making, and protects clinicians through proper legal documentation. Done poorly—or delayed—it increases risk, disrupts continuity and communication, and adds to the growing documentation burden across modern healthcare.
This article explores the past, present, and future of medical charting — from paper records to an AI scribe for medical charting — and how smarter tools may finally make patient charting easier for clinicians.
What is a medical chart?
Medical charting is the process of recording patient information, clinical observations, diagnoses, and treatments in a patient record. This documentation forms the backbone of modern healthcare.
At its core, patient charting tells the story of a patient’s care. Clinicians use charting to record patient history, treatments, and decisions made during encounters.
Dr. Jill Moes writes in Op-Med that medical charts are how she holds onto the human side of medicine in a sea of demands.
“Rather than just a rote history of clinical data, they can in fact be a detailed record of who my patient is and what really matters to them.” — Dr. Jill Moes
The components of a patient's medical chart include:
- Individual patient demographics
- Medication administration
- Medical history
- Treatment plan
- Test results
- Informed consent
- Progress notes
- Referral notes
- Patient narratives
Each element contributes to accurate documentation that helps clinicians understand the patient’s current condition and previous care. Without consistent medical charting, critical patient information can be lost, which undermines continuity of care and complicates clinical decision making.
Why medical charts are crucial in patient care
Imagine a patient arriving at the emergency department with a severe allergic reaction.
Without a medical chart, every doctor’s visit is a guessing game. The care team may not know the patient’s allergy history, medications, or previous reactions. Good charting prevents these dangerous knowledge gaps. Effective medical charting supports several core functions in healthcare:
1. Continuity of care
Clinicians rely on charting to maintain continuity of care across providers, departments, and facilities. Clear patient charting ensures that the next clinician can quickly understand what has happened and what should happen next.
Well-organized chart sections allow clinicians to quickly locate patient information, review progress notes, and assess treatment outcomes. This supports strong continuity and communication between care teams.
3. Legal compliance and risk management
Medical records also serve as legal documentation. Detailed patient charting protects clinicians and organizations through proper legal compliance and risk management.
Courts and regulators often rely on accurate documentation to evaluate whether appropriate care was delivered. According to one Harvard study, 20% of medical malpractice cases involve at least one documentation failure.
Poor or missing charting can expose clinicians to liability. For that reason, timely documentation and clear and concise language are considered essential best practices in modern healthcare.
A brief history of medical charts
Humans have recorded injuries and illnesses for thousands of years. Over 15,000 years ago, humans documented injuries (likely from an animal attack) on cave walls.
These primitive records were early attempts at charting—a way to document patient information and track outcomes. Over time, physicians began recording more detailed, formalized patient history and treatments with more objective language.
Paper charts: The start of systematic records
Paper charts, notorious for their unreadable handwriting, were the gold standard from the 1800s to the late 20th century.
They were simple, cost-effective, and immune to cyberattacks, but they had major downsides: storage was a nightmare, they got lost easily, and deciphering notes sometimes felt like cracking an ancient code.
Despite these issues, paper charting allowed clinicians to document care using clear and concise language. As Dr. Woojin Joo put it in his newsletter, they reminded him that patient care only requires three things: clinical knowledge, a pen, and paper.
The rise of electronic health records: Secure documentation at scale
The transition to digital records marked a major shift in medical charting. The EHR (electronic health record) allowed organizations to store and share large volumes of patient information across systems.
EHRs introduced standardized chart sections, searchable documentation, and digital patient charting tools. By the 90s, many hospitals had EHRs. By 2009, they were mandated.
Adoption skyrocketed, growing eight-fold in six years, with 90% of hospitals and 80% of physicians now using them for the medical record.
Data-driven health: Intuitive, user-friendly charts
Today, EHRs helped clinicians make medical charting work for scaled systems — but AI, big data, and automation are helping clinicians make medical charts work for them.
Instead of simply digitizing records, these technologies analyze information, actively assist in document creation, and even anticipate needs. These include:
- AI medical note tools that listen to patient visits and automatically generate clinical notes.
- Machine learning algorithms that detect early signs of disease from medical records.
- Speech-to-text AI that enables hands-free charting.
- Cloud-based platforms that break down data silos for seamless sharing across medical records.
Challenges of modern medical charts
While the EHR (electronic health record) improved access to patient information, it also increased the documentation burden placed on clinicians. The modern documentation burden in healthcare comes from several factors:
- Complex billing requirements
- Regulatory legal compliance
- Detailed legal documentation
- Administrative reporting
Clinicians report spending half their day on documentation, multi-tasking between patient and computer.
“There are patients who feel that their health care providers aren’t able to pay full attention to the patients themselves because the doctor is consumed by this technology,” — Dr. Steven Stack, AMA, US News.
Common challenges include:
EHR usability and clinician burnout
In many systems, simple charting tasks require multiple steps. Checking lab results may take several clicks. Updating medication administration requires navigating multiple tabs. Even locating key patient information inside the EHR can take longer than expected.
These small inefficiencies quickly compound. Over the course of a day, clinicians may spend hours navigating the EHR just to complete routine documentation. One study by Mayo Clinic found that the loss of control clinicians feel from poor EHR usability is one of the biggest contributors to burnout.
Documentation overload
Many clinicians feel pressure to produce extensive patient charting in order to meet billing requirements, support legal compliance, and maintain accurate documentation.
When clinicians rush through medical charting at the end of the day, they may resort to copying and pasting text between chart sections or writing excessively detailed progress notes. This type of documentation often buries the most important clinical insights and makes it harder for other providers to quickly review patient information.The result is longer notes and less clarity.
Interoperability challenges
Another major challenge in patient charting is the lack of interoperability between systems. When different organizations use incompatible platforms, continuity and communication suffer.
Clinicians may need to manually re-enter documentation or request records from other providers.
Without better interoperability, medical charting becomes fragmented across systems instead of supporting the coordinated healthcare patients need.
Best practices for effective medical charting
Improving patient charting does not always require new technology. Many improvements come from following proven best practices.
1. Use clear and concise language
One of the most important best practices in medical charting is using clear and concise language. Notes should focus on relevant clinical facts and avoid unnecessary detail. Write notes with the goal of making it easier for patients and/or other clinicians to understand.
2. Maintain objectivity
Clinicians should always use objective language when writing progress notes. Avoid subjective statements. Instead, focus on measurable observations. For example:
- Poor charting: “Patient seems uncomfortable.”
- Better charting: “Patient reports pain level of 7/10.”
Consistent objective language improves accurate documentation and strengthens legal documentation.
3. Record vital signs consistently
Clinicians should record vital signs during every appropriate encounter. Proper charting of vitals supports clinical decision making and helps identify trends. Typical vitals to record vital signs include:
- Blood pressure
- Heart rate
- Temperature
- Respiratory rate
Failure to record vital signs can create gaps in patient charting.
4. Document in real time (or as close as possible)
Whenever feasible, complete documentation during or immediately after the encounter rather than at the end of the day. You may want to use an ambient listening aide to help capture notes simultaneously while you conduct patient visits. This reduces omissions, improves accuracy, and creates a clearer temporal record of what happened when, which is useful both for clinical handoffs and in any future legal review.
SOAP charting: A common clinical format
One of the most widely used formats for patient charting is SOAP charting. SOAP charting structures clinical notes into four parts:
- Subjective
- Objective
- Assessment
- Plan
Clinicians rely on SOAP charting because it promotes organized chart sections and consistent documentation.
For example:
- Subjective: Patient reports symptoms and relevant patient history.
- Objective: Clinician observations, including record vital signs and exam findings.
- Assessment: Diagnosis and interpretation supporting clinical decision making.
- Plan: Treatment plan, follow-up care, and medication administration.
Many clinicians prefer SOAP charting because it improves continuity of care and supports accurate documentation.
How AI is transforming charting
AI is changing charting from a manual, click-heavy task into a more automated, conversational workflow. The table below highlights concrete ways AI tools reshape documentation and why those changes matter at the point of care.
The future of medical charts
We’ve seen how far medical charts have come — but there’s a long way to go.
From AI-led workflow enhancements to voice-assisted documentation, and better interoperability, this new wave of technology is bridging the user experience gaps that have made digital charting so cumbersome for clinicians.
- AI medical scribes: AI scribes like Freed turn patient conversations into structured notes—so clinicians can finish charts faster."
- Interoperability solutions: New frameworks help EHRs talk to each other—so clinicians don’t waste time on manual work
- AI chart audits: Platforms like SmarterDx help hospitals automatically scan medical records for documentation gaps before insurance claims are submitted. This helps CDI as hospitals address issues before it impacts revenue or compliance.
- Automated medical coding: This technology uses AI to convert physician notes into standardized diagnostic codes. It reduces errors and relieves clinicians of the burden of entering codes.
Smarter tech that helps clinicians do simple things better
For generations, clinicians have relied on charting to capture the story of patient care. From handwritten notes to the modern EHR, the goal of medical charting has always been the same: document patient information clearly enough to support treatment, enable clinical decision making, and ensure continuity of care.
The transition from paper charts to EHRs had its weaknesses, but that experience taught us that technology is only as good as its usability.
The next wave of innovation is about removing the busywork EHRs created.
These new tools are here to make medical charts more intuitive and human-centered, not to make clinicians feel like they have to learn another system.
Spend less time charting with Freed
Freed was built around a simple idea: clinicians shouldn’t have to choose between great patient care and finishing their notes.
Freed listens during patient visits and automatically generates structured clinical notes, so you can walk out of the room with documentation already drafted and ready to review. No late-night charting. No scrambling to remember details hours later.
Clinicians use Freed to:
- Finish notes dramatically faster
- Stay fully present during patient conversations
- Reduce after-hours documentation
- Produce consistent, high-quality notes with minimal effort
The result is simple: less time typing, more time practicing medicine.
FAQs
Frequently asked questions from clinicians and medical practitioners.
What is a medical chart used for?
Is a medical chart a legal document?
How can I find my medical chart?
What is the chart used in hospitals?
.avif)
Related content
Free yourself for better things
548 Market Street, PMB 95301
San Francisco, CA 94104
Specialties
Compliance & Security
Our technology is HIPAA-compliant, uses industry best practices, and doesn’t store patient recordings.